Social Media: 

 Website
Colour:
Website
Colour:
 -
-  -
-
|
ABOUT THIS BRIEFING: This briefing provides an overview of novel psychoactive compounds or “Research Chemicals” in the UK. It is not intended to provide detailed information on each compound or a list of all such compounds. Where substances have become sufficiently popular or enough is known about them separate briefings will be available on the KFx site and elsewhere. Look up charts of key drugs are also available on the KFx site. The web version has fewer images in it; the downloadable PDF includes more images, including statistics and schematics. This is version 2.1 rewritten July 2016 to reflect changes as a result of PSA 2016.) |
AKA:
Generic terms: “Legal Highs,” “Legals, “Herbal Highs,”
“Research Chemicals,” party pills, Novel Psychoactive Compounds, NPCs, NPS,
RCs, Designer Drugs
Generic Slang terms: Monkey dust, Bubble,
BubbleLuv, Pulse, Plant food, Bath Salts, Incense, Mamba, Spice, and many
others
Chemicals include: 4-MMC, Ethylphenidate, AMT, 1P-LSD, MDAI, MPA, 5-FMP,
AKB-48 and many others.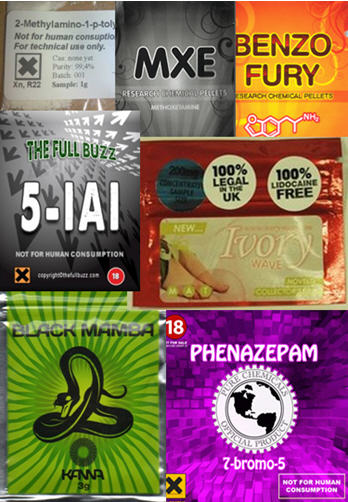
Terms
and Frame of Reference: Lots of terms
are used to refer collectively to NPS, some better than others.
The term “legal highs” was always dubious and with
the passage of the Psychoactive Substances Act is now wholly obsolete.
Even before the law changed, the term was
unhelpful. “Legal” has connotations of substances being licensed or regulated
which of course was not the case. They were unregulated: legal by omission not
permission.
Novel
Psychoactive Substances: This is the
term preferred by policy makers, Academics and some drugs workers. Novel Psychoactive Substances (or
Compounds) is typically shortened to NPS or NPC.) It’s a bit of a mouthful, and
hasn’t caught on with actual users. Pedants
would argue it’s not wholly accurate as not
all the substances of interest are truly “novel.” 4-MMC for example was
probably first synthesized in around 1929. Nitrous Oxide has been used for
almost 200 years. They may well be new to market but they’re not all new to
science.
Research Chemicals: On a lot of user-led discussion
forums, “Research Chemicals” is commonly used. Some chemicals were being
used in research settings and have started to appear recreationally. Before the
PSA shops sold products for “research” rather than human consumption as a legal
workaround. Some users like the terms as
they would rather view their use as being an intellectual “research” pursuit
rather than a hedonistic quest to get intoxicated. Whatever the reason the term
“Research Chemicals” is more familiar to some users than NPCs.
NOMENCLATURE: Newer drugs may end up with a confusing array of
names, making it hard to know which substance people are talking about.
Chemical Names: Drugs
will have a long chemical name. Some will have more than one as there may not
yet be an agreed chemical name. The “official” one is the IUPAC name, but not
everyone will use it. It describes the chemical structure.
The long chemical name may well be shortened to a short chemical name – often
based on the initials.
If a drug comes to market and becomes more popular it may end up with a more
user-friendly shorter name.
When drugs were being retailed via Headshops and on-line stores, different
companies produced “branded” products so people may refer to these rather than
the chemical or drug name. The same branding phenomenon occurs with some street
drugs, such as MDMA pills.
Finally, some compounds may end up with slang names, popularized by end-users
or in some situations by the media.
|
Common
Drug Name |
Chemical
Name |
Abbreviations |
Brands |
Slang |
|
Mephedrone |
(RS)-2-methylamino-1-(4-methylphenyl)propan-1-one (IUPAC name) 4-methyl-N-methylcathinone 2-methylamino-1-p-tolylpropan-1-one |
4-mmc |
|
Meph Bubble Miaow Miaow |
|
Ecstasy |
(RS)-1-(1,3-benzodioxol-5-yl)-N-methylpropan-2-amine
(IPUAC) 3,4-Methylenedioxymethamphetamine |
MDMA |
Mitsubishi Minions |
E, |
Chemical Names: The drugs in question will have a long chemical name. Some will have more than one as there may not yet be an agreed chemical name. The long chemical name may well be shortened to a short chemical name – often based on the initials.
So for example 4-mmc had at least three different long chemical names:
early ones were:
4-methyl-N-methylcathinone
and 2-methylamino-1-p-tolylpropan-1-one. Later the name
(RS)-2-methylamino-1-(4-methylphenyl)propan-1-one became the standard name.
The
abbreviation 4-MMC was an abbreviation of the long chemical name: 4-methyl-N-methylcathinone.
As it came to market, and started to get used and sold more, a more user-friendly
name was required and it was dubbed “mephedrone.”
Again this wasn’t a standardized name. It’s just some people
involved in the drug thought the name was a fair summary of the drugs structure
and name and it stuck. Others thought it was a lousy name, and argued, unheeded
for more “accurate” names, such as 4-MMC were suggested.
Some
retailers will now attach long chemical names to make a bogus product sound
like a real thing- by dazzling people with a very small amount of science,
such as the product E2 illustrated here:
Brand
Names: Before the
Psychoactive Substances Act came in, retailers were importing drugs, bagging and
selling them in branded packages. Rival companies would copy successful brand
names but their own product may contain different drugs of different strength.
Now that such retailing has effectively been
outlawed by the PSA, the vast number of branded products have been pulled from
the shelves, but some of the “brand names” persist so people for example still
talk about smoking “spice” or “mamba.”
A few brand names have become sufficiently
widespread that they have become generic slang. So for example there was once a
synthetic cannabinoid product sold as Spice.
It contained the chemical JWH-018. This form of Spice is long gone but the term
“spice”
has persisted and is now a generic term for synthetic cannabinoids, especially
in the prison system.
Plant Foods: In order to
get around the Medicines Act, and to reinforce the idea that the substances
were not being sold for human consumptiomn, some compounds were sold under the “cover” of being plant foods or bath salts. These slipped in to
general use as a blanket term for some NPS.
As newer products came to market, more cover terms have been employed including
pond cleaner, fish tranquilliser, incense
and pot-pourri. In
much U.S. coverage of NPS, the term Bath Salts has been used a huge amount in
the media and by commentators. The snag with such terms is they create
confusion: some naïve users believe
specific plant foods or bath salts are psychoactive.
This is especially confusing when some genuine
products (e.g. certain nail varnish removers, whipped cream propellants,
various medicines) do have the potential to intoxicate if misused.
User and Media Slang: The term Mephedrone was shortened to ‘drone, and some, especially the media, called
it Miaow Miaow.
Regional slang terms such as Monkey Dust or Bubble emerged.
These are often used as a generic reference to white stimulant powder drugs,
where the active contents are unknown. In the same way that “E” related to MDMA,
so “bubble” was originally slang for
a preparation on sale in the north of England containing 4-MMC and MDPV. Later,
just as E became a generic term for “a
pill that I necked in a club, not sure what’s in it but hopefully it will be a
bit speedy and trippy,” so Bubble
became a generic term for “a white powder
that I bought and I’m not sure what’s in it but hopefully it will be a bit like
‘drone but here goes…”
Other
“Herbal Highs,” and “Ethnobotanicals:”
There are a few herbal substances, that weren’t new.
hadn’t been regulated and weren’t that widely used. They now fall under the Psychoactive
Substances Act if sold for intoxication.
These are psychoactive plants or plant extracts. Some have cultural or ritual
use and are sometimes called “ethnobotanicals,” especially if it has elements
of spirituality or new-age mysticism attached to it. Peyote cactus, with
its associated sacramental use by American Indians, often ends up being
called an ethnobotanical. Khat despite
being botanic and associated with distinct ethnic groups doesn’t usually get
called an ethnobotanical. Presumably because it’s not mystical enough. Other
plants have no such rituals attached to them, but may also end up being called
ethnobotanicals.
Some of the ethnobotanicals contain substances
which, if extracted, would constitute a controlled drug. For example, the plant
Chacruna (Psychotria Viridis)
contains the hallucinogenic compound DMT. Chacruna is used in the South
American hallucinogenic brew Ayahuasca. Chacruna is legal to supply provided
such supply doesn’t fall foul of the Psychoactive Substances Act. A small
number of on-line suppliers do offer it for sale, and there are still vendors
offering plant extracts which is likely to be a breach of the PSA. DMT itself is
a Class A controlled drug, and people have been prosecuted for making brews with
Chacruna as it is can be considered production of a Controlled Drug.
Other plants, such as Salvia Divinorum are
now regulated by the Psychoactive Substances Act 2016.
The plants are generally grown abroad and imported
in to the UK. Excessive cropping for the international drug market has
increased cost and reduced availability. There is no quality control to
‘guarantee’ the identity or potency of substances being sold, and so the
plant-based products being sold could contain a different substance, or no
psychoactive compounds at all.
Some plant-based legal substances can have
unpleasant and possible dangerous effects. There’s a small and less-commonly
used collection of plant-based compounds which are notorious for being risky
and having unpleasant side effects. These include plants such as Henbane and
Datura which contain the psychoactive and toxic chemicals Hyoscyamine
and Atropine.
Most plant-based products will be covered by the PSA
if sold for the purpose of ingestion and intoxication. High availability on
line reflects paucity of enforcement rather than the plants remaining legal.
Medicines: a small number of Pharmacy Medicines (e.g. those
containing codeine) or substances with legitimate non-medical use (e.g. nitrous
oxide, Buscopan) are also used for their psychoactive properties. Although
not really NPS in the usual sense of the term they are included here as the
patterns of use are relatively novel.
The Backstory: The world of recreational drug use has never been
static. New substances constantly emerge. Coca leaf was the NPS of its day. Later,
cocaine was extracted and refined from the leaf, it in turn became an RC, used
for genuine experimentation and recreation. Rather than today’s psychonauts and
web discussion forums being at the cutting edge of drug experimentation, people
like Sigmund Freud and the upper echelons of society were pushing the drug
boundaries.
In truth, wholly new substances had been thin the
ground for a while. Prior to the early Eighties, outside of those with good
connections to post-graduate chemists with well-equipped labs, drug users in
the UK had the tried and tested opiates, LSD, magic mushrooms, cannabis,
benzos, amphetamines, and for the well off, cocaine. Plus solvents, if you had
to. Legal alternatives were promoted. A stroll around the less salubrious ends North
London’s Camden Market in the 90s would reveal a range of “smoking mixtures.” These
were typically blends of herbs with a reputedly cannabis-like effects but would
generally have all the intoxicating properties of a small bonfire and a similar
aroma.
So when Ecstasy (MDMA) arrived in
the UK in the mid-eighties, it was the first really ‘new’ drug to hit the
recreational scene in a fair while. MDMA was (being pedantic) not that new, having
been discovered way back in 1912. It was another 65 years before it was
“rediscovered” by Alexander Shulgin and another ten years before it became a
popular club drug.
If MDMA was the first major NPS, another key part of
the story of NPS was Shulgin’s magnum
opus Pikhal, a book describing the synthesis and effects of a large
number of drugs in the phenethylamine family.
The next key development was the explosive growth of
the World Wide Web. On-line communities emerged where people with an interest
in making or taking newer drugs could share knowledge and experiences. More
recently, it has allowed people to sell and buy new (and old) compounds with
relative impunity.
With Ecstasy dropping in quality fast in the UK
people looked for an alternative clubbing drug. A compound called BZP,
one of the piperazine family, was at the time legal and became briefly popular.
After MDMA it was probably the next proper “NPS.” It was made a Controlled Drug
in 2009. Others tried out, with varying degrees of success, GHB (not a great
clubbing experience) ketamine (ditto) and a range of other less familiar and
relatively new compounds.
Then somewhere around 2008, with a shortage of both cocaine and MDMA, 4-MMC (‘Mephedrone’) arrived. As a new, legal,
effective, cheap drug, it reached high levels of popularity in the UK. It reached
a peak in around 2010 when it was made a Controlled Drug.
The pieces of the jigsaw had come together:
underground chemists with the knowledge to make new compounds, bolstered by the
collective mind of some drugs forums, with the technological might of Chinese
and other labs happy to making the new compounds, and a ready market of
net-savvy end users willing to research, order and pay for the new compounds
on-line.
The
natural history of a Research Chemical: Emerging NPS, like mephedrone, had
an interesting life-cycle which has evolved over the past few years and will
change again as a result of the PSA.
Often, a chemical had been identified by scientists or
in the past. Some had been patented by pharmaceutical companies in anticipation
of their medical use. They then languished, unused, in old journal
articles and patent files for a number of decades. A small number of keen
post-grads might synthesize these for personal use, but they wouldn’t reach a
wider audience.
Eventually, a
particularly popular compound might start to grow in popularity and
availability. Initially this was underground, maybe not being discussed on
bulletin boards yet, and certainly not being marketed on-line.
After a while, through forums and underground drug
markets, some of these chemicals start to get produced in larger quantities.
Labs may be commissioned to produce the drug in bulk. At this stage use becomes
more extensive, the media and wider world becomes aware of the substance.
Finally after the drug comes to wider media and Government attention, it is
likely to be added to the list of Controlled Drugs. There may be a “tail” of
use as residual drugs in the system are used up. If the substance was
especially popular or effective, it may continue to be made and distributed but
through more traditional street markets rather than on-line selling. However,
it seems that with the majority of NPS, their key market advantages were cost,
legality and availability. Once banned, the majority drop out of the market.
6-APB (‘Benzo Fury’) was one of the post-mephedrone NPS widely hyped by
retailers. It was made a Controlled Drug and vanished from the market place.
Newer
products coming to market: After the heady
days of mephedrone, the market changed a great deal. New products were still
coming out quickly. Some, like JWH-018 or Ethylphenidate jumped from research
settings to the recreational market. Some were older compounds (e.g.
phenazepam) and others were brand new, designed drugs (e.g. 5F-AKB48).
Key websites were quick to expand their range. MDPV, Naphyrone and other drugs
were added to the roster of products on sale, whether or not they were yet
available. Lots of websites highlighted that products would be “coming soon,”
and encouraging people to register or offering samples.
The extent to which these compounds were genuinely available or going to be
available is hard to judge. By the time Naphyrone (NRG-1) had started to emerge
and been made illegal, the next generation of compounds like NRG-2 and NRG-3
were being touted – and all the evidence indicates that these were wholly
fictitious compounds.
“Proprietary blends” with interesting brand names
were flogged via numerous websites and in a fair few pubs and clubs. Some of
these contained little or no psychoactive material. White powders could contain
caffeine and lidocaine which will give a mildly stimulating effect plus some
nasal numbness, and thus can be passed off as a cocaine-esque research
chemical. It could equally be a mix of old, now banned research chemicals or
there may simply be inert material pressed in to a pill. Without lab analysis
we couldn’t know. For example, a study published in 2011 analyzed seven
compounds bought from online retailers in the UK. Six out of the seven samples
didn’t contain the advertised compound, and five of the seven contained banned
controlled drugs.
The on-line retailers could be accused of killing the golden goose: by offering and making claims for a growing name of poor quality products, those with money and sense became increasingly wary of on-line retailers.
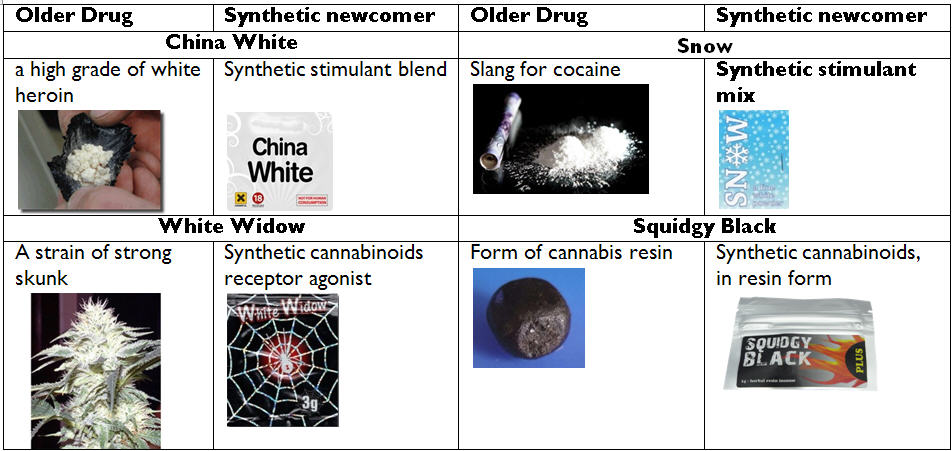
Leftovers: As individual drugs were
prohibited, leftover products remain in the marketplace.
Some left-overs got combined with currently legal,
or inert compounds, were repackage, relabeled and sold through “legal high”
channels as a new “legal” high. Lots of newly-banned MDPV ended up being sold
as the then-legal drug Naphyrone (NRG-1). People who thought they were getting
“legals” were in fact buying controlled drugs.
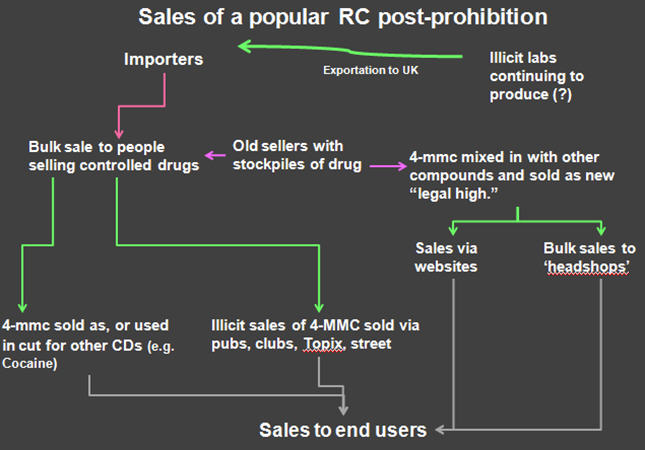
Some (more popular ones) continue to be sold by
name. So sales of mephedrone continued after it was made a Controlled Drug in
2010. It’s not clear how much “new” mephedrone has been manufactured or
imported since then, and how much pre-ban mephedrone was already in the system.
Residual mephedrone was bulked out or mixed with
other white powders. So when newer users (who started use post-ban) say that
they are using “mephedrone,” it may
well be that they are using any one of a range of substances. It could be
mephedrone, another new compound sold in place of mephedrone, or something
else. In one area young people were being sold speed as ‘mephedrone.’
It’s probably better, if people say they are using
mephedrone, to mentally interpret this as being an “unknown white powder.” It
certainly won’t be pure mephedrone.
Other white powders were sold on to old-school
dealers and started to appear in place of, or as a cut in existing CDs. So MDPV
may turn up in place of MDMA, MPA in Speed and Methoxetamine was passed off as
ketamine.
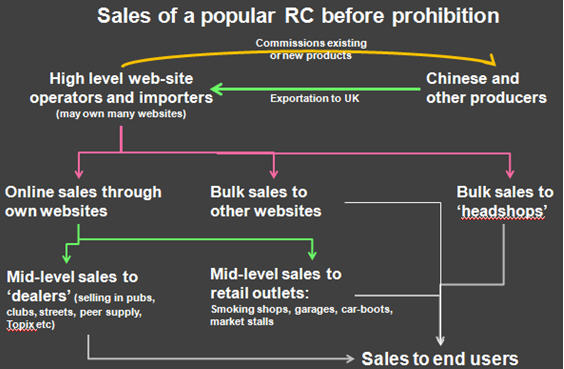
Production:
The NPS market in part follows traditional drug
markets but is also intrinsically linked to web-driven global markets. It is
simultaneously old-fashioned but at the cutting edge of technology.
There are different stages to any drugs market. So
for example when 4-MMC was widely available and legal the model looked
something like this:
We don’t know where each NPS is
produced. Some were produced in mainland Europe and some possibly in the UK. Significant
amounts came from China. Sometimes, Chinese labs developed new products
themselves (or at least claimed to.) In most cases labs offered to produce new
products for international vendors. Purchasers arrange to buy product, may
visit a lab to sample product or inspect the process and then drugs are shipped
internationally to the purchasers.
A development that eased this process was the emergence of international
trade websites such as Alibaba. This
made it easier for purchasers in the UK with little or know knowledge or
experience of dealing with Chinese laboratories to find producers willing to
produce NPS.
Markets and Marketing:
Pre Psychoactive Substances Act, a number of markets
had emerged:
Forums: When 4-mmc newer drugs first appeared distribution
was relatively clandestine. Supply took place via forum personal message.
On-line
shops: At this stage, many NPS were still unregulated and
so were openly sold on-line. At first there were a small number, but by late
2009-early 2010 there was a huge growth in the number of these sites.
Most of these appeared quite professional, with capacity to take payment by
credit card, shopping-cart technology and claims made for the purity of the
drugs. For anyone with start-up capital, the ability to source product from
China and the knowledge to set up a website, this was an unparalleled chance to
make money quickly.
We don’t know how many different people were
involved in this. Some individuals undoubtedly controlled numerous websites
selling the same products through different sites. One individual controlled in
excess of sixty different web domains ready to sell compounds.
As this process escalated, some people set up
on-line but with no product at all – and so ended up bagging and selling other
things – caffeine, inert powders and so on.
Classic
markets include peer-to-peer supply and low level dealers
buying bulk on-line and then redistributing at a street level and via pubs and
clubs.
Retail outlets have been a key sales point for NPS. Initially this
was primarily “head-shops” and similar but as the market expanded, more and
more outlets joined in. This has included tattoo parlours, sex shops, fast-food
outlets, corner shops, market stalls, car boot sales, and, according to a
couple of correspondents, even petrol stations.
Other
markets include an
increase in selling via other websites, including Topix, Facebook
and other social media. However, such arenas
attracted a high level of scammers. Dark-web sites such as Dream Market do sell
some NPS but the bulk of the product for sale remains “traditional” controlled
drugs and more esoteric psychedelics.
Google,
Sock Puppets and Forums: In 2009, a
Google search was the easiest way to find an on-line NPS retailer. Google AdWords
programme would promote vendor websites in response to search terms such as
Plant Food, or Mephedrone. At some point a decision was made to end this
advertising.
New drugs got discussed on drug-discussion forums
such as Bluelight or Drugs Forum. Both prohibit naming specific websites and
on-line vendors. On one hand this prevented promoting sites. Unfortunately, it
also meant they couldn’t out the “rogue” sites selling bogus products.
This forum self-censorship on these websites drove suppliers to
less-well-moderated websites and forums. A key promotional tool on such sites
was the “sock-puppet,” where a retailer creates several alternative identities
who can then converse, extol the benefits of a new product, say how reliable
they find specific vendors and so on. Such Sock Puppets are generally removed
from Drugs Forum and Bluelight, but on other sites promoting NPS, the majority
of accounts seemed to be Sock Puppets. This made it harder to sort fact from
fiction in discussion forums.
LAW:
In May 2016
the Psychoactive Substances Act came in to force, as a response by Government
to the use of NPS. Prior to that a number of piece-meal measures had been used
to control the market including:
Concerned that the existing measures were not
addressing the issue, the Government proceeded with a blanket-ban approach.
The Psychoactive Substances Act[1] creates Criminal and Civil
Powers to control the production, importation, export, supply, possession with
intent to supply and possession in custodial settings of any
psychoactive substance (unless exempt.)
The legislation effectively made the sale of NPS by
Headshops and on-line retailers illegal overnight. Because it covered any
Psychoactive Compound, the process of tweaking molecules to bypass a legal definition
ceases to be a solution, as does creative “not for human consumption”
labelling. If it’s demonstrably psychoactive, and not exempt, it’s covered.
The legality of substances will vary on a drug-by-drug basis. Some are specifically covered by the Misuse of Drugs Act e.g. 4-mmc. Others are not currently Controlled Drugs and but will instead be covered by the Psychoactive Substances Act. At some point, drugs covered by the blanket PSA may be added to the Misuse of Drugs Act.

Schedule
1 controlled drugs: these are not
currently held to have any medical use and so outside of possession by law
enforcement or Home Office-licensed researchers, possession will generally be
illegal. This includes drugs like LSD and MDMA and newer drugs like Mephedrone.
Schedules
2, 3 and 4i: these are controlled drugs but
also Prescription Only Medicines. Outside of professionals authorized to
possess them, it will be lawful to possess them if they are prescribed to you,
and some other specific circumstances. Methadone, buprenorphine and diazepam
are in schedules 2, 3 and 4i respectively.
Schedule
4ii Controlled Drugs: Anabolic
steroids and other performance enhancing drugs fit in to this Schedule.
Possession without a prescription is not an offence, although supply is.
Schedule
5 Controlled drugs: A small
number of Controlled Drugs (including codeine and morphine) are legal to purchase
from Pharmacies and possess without prescription in certain formulations (e.g.
codeine-paracetamol tablets containing 8mg codeine.) These are the subject of
significant misuse in the UK.
Temporary
Class Drug Orders: There was concern that process of new products
coming to market, the ACMD being able to research it and a decision Schedule it
was too slow. New legislation was passed to allow drugs to be temporarily added
to the list of Controlled Drugs, pending review by the ACMD and decision on
scheduling.
Temporary Class Drug Orders (TCDO) came in to force
in 2011. Drugs can be placed in this category by the Home Secretary. This makes
it an offence to produce, import or supply the drug, and offences carry a
maximum of 14 years imprisonment and/or unlimited fine.
Possession of drugs subject to a TCDO is not a criminal offence. As all new compounds are automatically covered by the PSA, and the new Act like the TCDO category restricts supply but not possession, it seems unlikely that many new drugs will be added to the TCDO list.
Analogue
clauses: once upon a time, drug legislation listed specific
compounds as being controlled drugs. As science has advanced, a drug-by-drug
approach can’t keep up with numerous molecular variants. An analogue clause is
intended to cover a range of compounds by describing the likely chemical
variants that could be produced based around the same core structure. So for
example in relation to some tryptamines, the legislation prohibits:
any compound (not being a compound for the time
being specified in sub-paragraph (a) above) structurally derived from
tryptamine or from a ring-hydroxy tryptamine by substitution at the nitrogen
atom of the sidechain with one or more alkyl substituents but no other
substituent;
Analogue clauses prohibit whole families of drugs
and potential future drugs. However, it does mean that we don’t always know if
a new drug is illegal or not. The wording can be so complex and technical that
few people with sufficient knowledge of chemistry will understand what it prohibits.
Further legal arguments would need to determine what the phrase “structurally
derived from tryptamine” means on a case by case basis.
New compounds had got around analogue clauses by departing sufficiently from
the prohibited structure, thus avoiding being “Controlled Drugs.” As the new
Psychoactive Substance Act covers all psychoactive structures irrespective of structure,
such molecular tweaks are covered by the newer legislation.
Pharmacy
Medicines: Similarly, there are a few pharmacy-only medicines
which are not controlled drugs, but also may be used outside of
medical settings. So for example the antihistamine diphenhydramine is
used for its psychoactive properties. Recently the misuse of Buscopan in
prisons has been a growing cause for concern.
Volatile
Substances: As part of the Psychoactive Substances Act, the
older Intoxicating Substances (supply) Act 1985 was repealed. This had made it
an offence to supply any substance to a person under 18 where the product was
to be inhaled for intoxication. The PSA also covers household products sold for
the purpose of intoxication, so the older law was no longer needed.
Borderline
Products: Some products contain psychoactive compounds or
those that have a medical use. Depending on how the products are processed,
packaged, labeled and promoted they may or may not be considered Medicines. The
Borderline Products Team within the Medicines and Healthcare Products
Regulatory Authority (MHRA) will consider such products to determine if they
should be considered medicines or not.
Those that are considered medicines will then be subject to all the
relevant regulations, and risk of prosecution for those who sell them outside
of these regulations.
Products which the MHRA hasn’t ruled on, or has
determined are not Medicines fall outside the Medicines legislation. So for
example, Nitrous Oxide may be packaged and sold as an anaesthetic. In such
situations it would constitute a medical preparation and would be regulated as
such. But the same compound sold (for example) as a propellant for whipped
cream would not be regulated in this way.
NPS retailers
avoided Medicines legislation by labelling products “not for human
consumption,” but such an approach isn’t usable against the Psychoactive
Substances Act.
[1]
There’s a separate KFx briefing on the KFx Website at http://www.kfx.org.uk/resources/PSA2016briefing.pdf
TRENDS: It is hard to get an accurate prevalence data on NPS.
Drug Misuse Declared is specifically concerned with Controlled Drugs and so
until a drug becomes a CD the CSEW doesn’t tend to look at it. Newer
uncontrolled compounds don’t feature in detail in the CSEW, and the overall
reporting levels of NPS are low, making it hard to see what impact newer
compounds are having.
To make matters worse, the speed with which new
drugs are identified and then added to the survey is relatively slow so
effectively drugs that come to market in one year and have been prohibited the
next year won’t end up accurately reflected in the CSEW.
Finally, with some new compounds, terminology and
geography may be very variable. Where drugs are concentrated in specific
regional pockets or where some drugs are only known by specific names, this may
not be well picked up by a broad piece of research such as the CSEW.
So based on the CSEW, the proportion of young people
aged 16-24 who reported mephedrone use in the 2012-13 was1.6%, down from 4.4%
in 2010-11, the year that it was made a CD.. The levels of use amongst regular
clubbers was higher.
In a self-reporting survey conducted by Mixmag in
2012, levels of mephedrone use were reportedly much higher. However, these
surveys are very highly selective and probably significantly over represent
levels of drug use just as the CSEW is liable to under-report use.
The Mixmag survey above reported 19.5% of UK respondents had used
mephedrone in the past twelve months, twice what the CSEW reported even for
frequent club-goers.
The survey also highlights the ongoing popularity of
“traditional” substances and the relatively low up-take of NPS even when they
were legal and widely available.
An interesting way of looking at trends in novel
drugs is to use a proxy indicator such as Google Trends. This can help to
indicate shifts in levels of interest in a drug. It seems reasonable to assume
that these shifts in interest trends will correlate with usage trends. This
doesn’t mean that interest equals use, but that ups and downs in interest may
well correlate with ups and downs in use.
When we look at interest in key novel psychoactives,
interest in MDAI started high and, although it remained unregulated until the
passing of the PSA, interest had tailed off significantly. Interest in
Ethylphenidate had increased until it was prohibited. There was more interest
in the drug Etizolam a benzodiazepine-type drug.
What is more striking is comparing relative interest
in 6-APB with mephedrone. What is evident from this is that interest in 6-APB,
even at its peak, is relatively low compared to interest in mephedrone. The
very tip of the 2010 mephedrone spikerepresents the furore of media interest
up to the point where mephedrone was made a controlled drug. But even
disregarding this spike, the peak in interest in mephedrone was far greater
than in terms of other new drugs. It appears that nothing since then has
generated the same level of interest.
Despite all the media interest in
NPS the substances were not as widely used as their traditional counterparts
with the exception of some key cohorts, such as in prisons, or amongst homeless
populations.
DRUG FAMILIES: There
are several ways of trying to classify drugs. We could split our drugs up by:
·
Chemical structure: this means that
families of drugs with similar chemical structures will be grouped together.
Some will have similar properties but there may be others which don’t. These
could be very broad families (e.g. the phenethylamines
would be a very large family, or smaller groups within the larger family – e.g.
the beta-ketones of which mephedrone
would be an example.
·
User-perceived effects: here drugs will
be grouped by how they are meant to make people feel. Alongside our
“stimulants” drugs could be “psychedelics” “dissociatives” or “empathogens.”
·
Pharmacological effect: this would look
at how the drugs are working at a brain-chemistry level. This can be especially
useful as it can highlight potential risks of a compound. But, especially when
a drug is new we may not know a huge amount about how it actually works.
·
The context in which they are used: for
example, to induce sleep, as a club drug or for profound hallucinatory
experience.
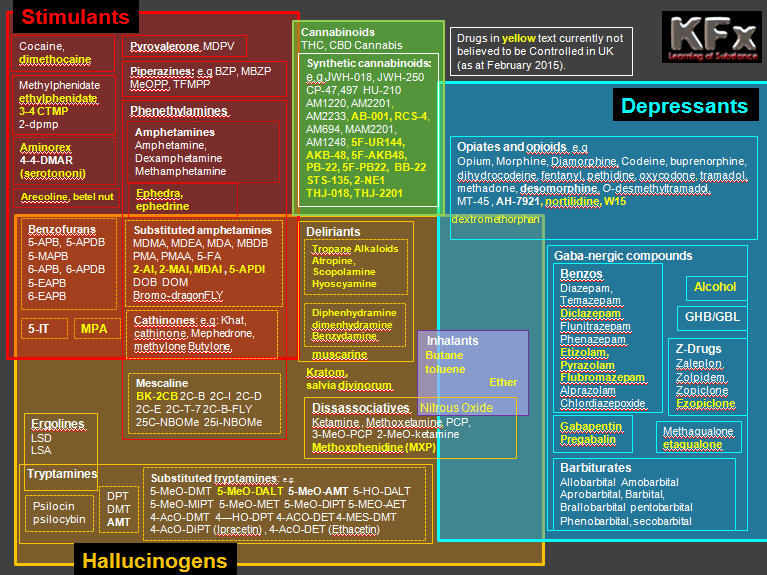
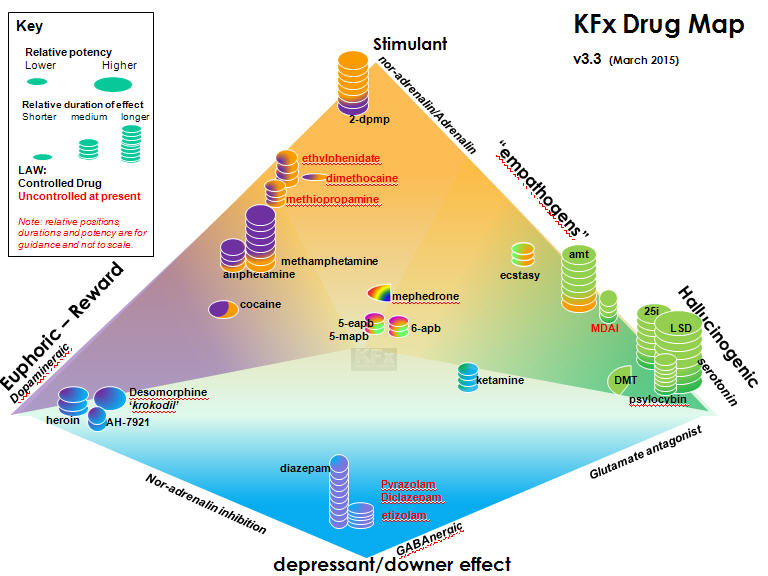
For
most people a model which draws on a bit of each model is useful. Having a
little bit of a grounding on the behind-the-scenes brain chemistry is very
helpful too. The schematic below locates some of the key compounds in terms of
effects and legal status.
Stimulant
Drugs elevate key neurotransmitters, including
nor-adrenalin, and possibly dopamine and serotonin. They could do this through different
mechanisms such as increasing release of and/or inhibiting reuptake of these
chemicals. The extent to which levels of a specific compound is elevated will
determine the effect. Drugs with elevate dopamine significantly will induce
greater reward and euphoria, but are more likely to increase a desire to redose.
Those that have only elevate nor-adrenalin will offer little euphoria, but may
increase alertness and cause anxiety. They also increase strain on heart and
circulatory system.
Hallucinogens
are drugs that have less stimulant activity
but significantly alter perception. Many of these work on serotonin receptors
in the brain. They may mimic serotonin or elevate serotonin levels by
increasing release and/or inhibiting reuptake.
Drugs which elevate levels of serotonin can be more hallucinogenic, and can also
increase feelings of empathy. The emotional closeness engendered by these drugs
sometimes earns them the name “empathogens.” Drugs such as MDMA fit in to this
category.
Other hallucinogenic drugs have different mechanism
of action and can feel profoundly different to serotoninergic drugs. So for
example the deliriants atropine and hyoscamine, found in certain plants, induce
hallucinations through a wholly different mechanism, and this is associated
with profound disorientation, disordered thinking and confusion.
Depressant drugs, as a term is
something of a misnomer, as they can also be significant euphoriants. They act
as depressants on the central nervous system, slowing down breathing and heart
rate, and inducing relaxation and drowsiness. Several drugs in this family act
on the regulatory neurotransmitter GABA, elevating or mimicking it.
Opiates work differently, by reducing levels of
nor-adrenalin and so having a calming effect. Combinations of depressant drugs
are a key cause of fatal overdose. They also tend to cause significant physical
dependency with extended use.
Synthetic
cannabinoids are also referred to as synthetic
cannabinoid receptor agonists. They bind to CB1 or CB2 cannabinoid receptors in
the brain and body. The chemicals THC and CBD in cannabis activate these
receptors and synthetic cannabinoids can do the same. Some are much more
powerful than THC and others have greater specificity to different receptors.
They can have a range of effects, and straddle the Stimulant/Depressant/Hallucinogen
as they have some of the characteristics of each.
COSTS: Massively
variable depending on drug, quantity, source and other factors.
QUALITY CONTROL: Even when NPS were unregulated, quality control was
highly variable. In response to seizures by Trading Standards, some suppliers
made efforts to ensure that packaged products were more accurately labelled.
Often, there was still significant variance in strength and quality.
In the wake of the PSA, residual product sold away
from shops isn’t hampered by Trading Standards or labelling. Left-over stock gets
mixed up and sold on, and so, for example generic “Spice” sold on the streets
could contain a mix of any synthetic cannabinoids. There is absolutely no
quality control at a street level and each new batch of synthetic cannabinoid
or white powder should be treated as an unknown substance.
DRUG
TESTING: Most
of the NPS produce different metabolites to those that are routinely detected
by urine test kit and so may give negative results. Even when more detailed
testing is done, some new drugs won’t be detected by most immunoassay tests as
the drugs haven’t been around long enough for such tests to become available. So
for example a new urine testing kit to test for synthetic cannabinoids came out
in July 2012 in the UK – but won’t test for all the new synthetics.
Even
if actual drugs are found, testing them using GC/MS testing to ascertain their
identity is complex as any testing needs to be compared against reference
samples. So typically a new substance emerges, a reference sample is analysed
and this forms the benchmark against which later testing is compared. For some
new drugs, where this hasn’t yet happened, compounds may not be correctly
identified or identified at all.
A small number of compounds produce sufficiently similar metabolites so may
trigger false positives on a urine test. High levels of 4-MMC use can result in
a false positive for methamphetamine use.
As
many drugs are blends of different compounds, positive testing may show up one
substance in a cocktail but doesn’t mean other non-detectable substances aren’t
present.
End
users, unable to access any such testing, may end up using chemical testing
kits available on-line. These change colour in the presence of different drugs
and allow people to partially identify some drugs to an extent. This is
somewhat hit and miss, and may not identify dangerous adulterants.
DOSES:
Given the newness of NPS, the
variability in quality and adulteration of street projects it is impossible to
speak with certainty about doses. Unlike traditional street-drugs, some very
potent drugs are sold on-line in very pure forms requiring minute doses to
avoid unpleasant effects. Conversely, other less potent drugs are being sold
which requires significant doses for any effect.
Whereas
amphetamines sold on the streets may have had purity of 5-10% products such as
MDPV were initially sold at purities in excess of 90%, meaning users needed to
rethink dosing with drugs of higher purity.
Dose
ranges will also vary according to the users’ body weight and their familiarity
with psychoactive compounds.
With
all novel compounds, users can’t tell if they are going to have an aversive or
allergic response to the drugs, so it can reduce risk if the person takes a
very small tester dose – below the level of an effective dose, to ensure that
this doesn’t cause a bad reaction. If this doesn’t cause an unpleasant
reaction, the person could then, after a reasonable time has elapsed, consider
taking a dose at the low end of the range for an effective dose.
As
some NPS are very potent even at low doses, high quality sensitive scales are
advised. However, good quality scales are expensive, and need to be correctly
calibrated. Given an entry-level set of laboratory scales will cost in excess
of £150, one must be wary of sites offering scales being sold by legal high
sellers for £20-30.
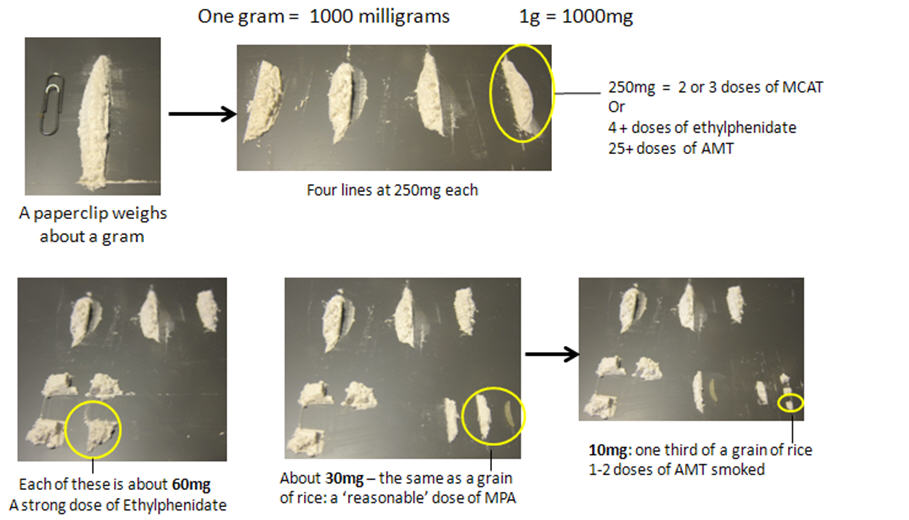
The
lack of good scales or, for that matter any scales means a lot of people will
try and judge their dose-sizes by eye – or “eyeballing” the drugs. So many
people will gauge doses by comparing to “a grain of rice” or divisions thereof.
Such an approach is of course highly risky, especially where people are using
drugs where the difference between a weak dose and a strong dose could be very
small.
When discussing or reading about doses, it’s worth double checking what units are being used. The abbreviation mg will be used a lot – short for milligram. It is important not to get milligrams mixed up with micrograms (mcg). So:
|
1
gram = 1000 milligrams 1 milligram = 0.001g 1mg = 1000 mcg (micrograms) 100mg = 0.1g 100mcg = 0.1mg |
METHODS
OF USE:
Routes
of administration will vary from research chemical to research chemical, and
person to person.
Synthetic
cannabinoids:
almost
invariably smoked. This may involve pipes, bongs or vapourisers. More commonly
the herbal smoking mixture is smoked with tobacco or another substance in a
spliff. There have been some reports of eating herbal preparations and a few
reports of snorting the raw powder but this is not typical.
Powder drugs (e.g.
mephedrone): As with other
powder stimulants such as cocaine, snorting is common. Lots of people
experienced significant pain when snorting NPS and some people experienced a
lot of nasal damage. To avoid these problems, swallowing (bombing) powder
stimulants has become much more common.
A
relatively small number of people take their powder stimulants rectally and for
some people seriously experimenting with new compounds it is a preferred route.
Some
of the powder stimulants (e.g. MDPV) are smokeable and there have been a few
reports of smoking becoming more popular.
As
most of the powder stimulants are water soluble, there have been reports of
injecting, discussed below.
Injecting RCs: Injecting is inherently risky. These risks
are still greater for NPS as we don’t know what is in them.
Incidence
of injecting is relatively low, and is primarily restricted to existing
injectors. However, reports from the UK and further afield have noted
significant problems amongst new and existing injectors using NPS. 4-mmc
(mephedrone) and other white powders were the main substances reported being
injected.
Some
of the people injecting 4-mmc or other research chemicals are experimental or
recreational users. Others are people who have been using NPS, whose use has
escalated and so use has migrated to injecting. This population are typically
not experienced injectors and the complications they have experienced may be a
result of inexperience, poor technique and hygiene as much as the drug itself.
The
other key population is existing injectors, especially heroin injectors who
have started injecting 4-mmc or other compounds instead of, or along with
heroin. These injectors have typically been more experienced but have still
presented with infections suggesting that this may be related to the drugs
themselves rather than injecting technique.
As
the main products are short-acting stimulants, injectors may end up injecting
more frequently and so expose themselves to greater risk.
Heavy
use of stimulants may impact on diet and general health, slowing down healing
and increase risk of infections.
If
working with people injecting RCs:
DEATHS:
As with the difficulty in establishing trends in
usage in relation to new drugs it is hard to establish rapidly and accurately
the number of deaths related to these drugs. Whilst the media and initial
reports are quick to report links to specific drugs when deaths occur, it is
hard to establish categorically which drugs were involved and the extent to
which they were a significant factor in any fatality. Especially with new
drugs, they may not have been tested for, or shown up in testing.
The most frequently recorded NPS to date has been Mephedrone was present in 46 fatalities and attributed as cause of death in 29 cases in 2010. This was an increase on the previous year. As mephedrone was made a controlled drug in 2010 and saw a subsequent decline in interest (and possibly use) there may be a resultant downturn in deaths in the next study. The rise in the use of Synthetic Cannabinoids is likely to mean this will feature to a greater extent.
Key Messages and Harm Reduction
regarding NPS:
As we (a) don’t know a huge
amount about NPS and (b) can’t be confident about what specific compounds
people are actually taking, it is not easy to offer specific harm reduction
advice.
We should really be very cautious about offering highly detailed information
about risk or risk-reduction as we don’t know enough to do so from a position
of robust evidence. We don’t know which compounds will turn out, for example,
to be highly liver toxic or which ones at low doses with cannabis could trigger
convulsions.
Given these significant
unknowns, harm reduction information needs to be couched in relatively general
terms until we can be confident that more specific and detailed information is
supported by some evidence.
Key messages: There are some general messages that are
applicable to all new compounds, irrespective of drug family.
·
As with older drugs, you don’t ever know what you are
taking
·
With newer drugs we don’t have the same “kept
knowledge” that we have with older ones, which means we can’t easily advise on
doses, likely effects and side effects
·
Specialists, including paramedics and addiction
workers, aren’t as familiar with newer drugs and this makes it harder to
respond in emergencies and when problems develop
·
Just because something is new, it doesn’t make it
safer than older drugs.
Key Harm Reduction:
1: Research: do
research first. Read up online. Read a variety of user reports. Use the better
websites which weed out shills and trolls and suppliers.
2: Think: do you really want to be a guinea pig with an unknown
substance?
3: Start with a very small quantity. Don’t try and gauge quantities by
eye, it’s too inaccurate. If you can’t access or afford highly sensitive,
correctly calibrated scales, don’t play with unknown drugs. Where possible base
initial dose at the low end of the active dose range, allowing for your body
weight where possible.
4: Don’t mix drugs: if you are trying an unknown compound, don’t mix it
with other drugs (including alcohol) or medicine.
5: Don’t do unknown chemicals unless you are in good physical and mental
health.
6: Have a friend with you who knows what you are taking, will not use
anything themselves, and will call an ambulance without any hesitation.
7: Don’t overdo it: Give yourself a good chance to recover before
redosing.
8: If you like the experience only increase quantities very slowly and
carefully.
9: Know the related drugs: Assume at the least that these compounds will
have similar risks to related compounds in the same family
10: Don’t supply compounds or bulk buy large amounts
EFFECTS and RISKS:
Drug Family Summaries: As we are covering a very large number of different drugs this briefing will not list and detail the effects of each. By grouping key drugs it’s possible to provide a summary of key effects and risks. More detailed information about some specific compounds is on the KFx website. (Colour coding as per Drugs Table)
|
Synthetic Cannabinoids |
|
|
aka
Synthetic Cannabinoid Agonist Receptors, Incense, Pot Pourri, Synth Canna |
|
|
Examples: |
Covered by PSA: AKB48, 5F-AKB48, PB-22, 5F-PB22 and numerous others. Covered by MDA
include JWH-018 and AM-2201. Pre-PSA brands included Exodus Damnation, Pandora’s Box, Clockwork Orange, Sensate, Psyclone.
|
|
Description: |
these compounds appear to mimic the effect of THC
at cannabinoid receptors. Some are more potent than THC. |
|
Route: |
Generally smoked either with or without tobacco;
also in E-Cigs. Rarely snorted or swallowed. |
|
Effects:
|
Generally, as for very strong cannabis including
euphoria, disorientation, stoned feeling |
|
Risks:
|
At lower doses, as for strong cannabis, including
panic, anxiety, dysphoria and confusion. More severe symptoms include
numbness of limbs, loss of consciousness, respiratory distress, severe panic
attacks, palpitations, acute mental illness, psychosis, hallucinations, nausea,
vomiting, convulsions, paralysis and rapid heart rate. A small number of
fatalities have been linked to use of these compounds. Some users report
long-lasting comedown and feeling depressed for several days afterwards. They
can cause tolerance and withdrawal symptoms, including severe stomach cramps,
sweats and pain. |
|
Harm
reduction: |
Use at very low doses, if at all. Dose sizes
should start no bigger than the size of a match-head. Don’t use in
conjunction with cannabis or other drugs. Avoid if prone to panic, anxiety or
mental health problems. |
|
Stimulants |
|
|
Examples: |
3-FMP, Ethylphenidate, MPA, camfetamine,
ephedrine, khat, amphetamines, cocaine |
|
Appearance |
White or off white powders; may be sold in wraps,
small self-seal bags, or printed foil bags old pre ban-stock). Substances may
also be sold in capsules or pressed in to tablets. Khat comes as fresh or
freeze-dried leaves. |
|
Description: |
Central Nervous System (CNS) stimulants with
little or no hallucinogenic activity. Some primarily elevate levels of
adrenaline and nor-adrenaline; others also elevate levels of dopamine. Those
with less dopaminergic activity will be less euphoric & rewarding. One
may be left with a more functional stimulant, which keeps you awake without
feeling especially pleasant. |
|
Route: |
Swallowed or snorted; rarely injected |
|
Effects:
|
As for amphetamine or cocaine – increased
alertness, reduced fatigue. Possible euphoria depending on drug. Increased
heart-rate and blood pressure. Reduced appetite. |
|
Risks:
|
As for other stimulants: damage to mucous
membranes through snorting. Risk of cardiac or circulatory problems. Weight
loss, insomnia. Risks of panic and anxiety, possible paranoia. Excessive or
extended use could trigger acute mental health problems. |
|
Harm
reduction: |
Use only at low doses. Avoid frequent redosing or
extended binges. Don’t use if any history or cardiac, circulatory or mental
health problems. Research in to new drugs prior to use to understand effects,
doses and risks. |
|
Hallucinogenic Stimulants |
|
|
aka
Empathogens, enactogens, psychedelic amphetamines; |
|
|
Examples: |
MDMA mephedrone
(4-mmc), 5-apb, 6-apb, MDAI, MDAT |
|
Appearance |
White or off white powders, and also pellet,
capsules and tablet forms. |
|
Description: |
Substances which have a mixed action including
some stimulant/euphoriants properties but also significantly alter
perception. This is usually because the drug elevates levels of serotonin by
increasing release and/or blocking reuptake of this brain chemical. |
|
Route: |
Mucous membranes (e.g. snorted), swallowed, rarely
smoked and injected. |
|
Effects:
|
Will vary widely from substance to substance, with
dose, user and context. Could include physical symptoms similar to other
stimulants (elevated heart rate and blood pressure, reduced appetite).
Altered perception, auditory and visual hallucinations, enhanced sense of
touch. Feelings of sociability and closeness to other people, sexual arousal.
May also include side effects such as reduced urine output, clenched jaws,
perspiration and restlessness |
|
Risks:
|
In addition to all the risks of stimulant use
(e.g. panic, anxiety, heart problems, insomnia, weight loss) other risks
include powerful changes to perception, intense feelings of panic and
paranoia. Drugs could elevate serotonin, leading to serotonin syndrome. This
could have a big impact on body temperature leading to overheating. Risk of
loss of circulation at the extremities. Risk of convulsions. Heavy use could
trigger episodes of psychosis. |
|
Harm
reduction: |
Use only at low doses. Avoid frequent redosing or
extended binges. Don’t use if any history or cardiac, circulatory or mental
health problems. Don’t use in conjunction with other drugs or medicines.
Undertake research to understand specific risks related to each drug being
used. |
|
Hallucinogens |
|
|
aka
Psychedelics, tryptamines |
|
|
Examples: |
LSD 2-ci, 2-cb,
dmt, 5-meo-dipt, 5-meo-dalt, 2-ai, amt, chacruna,
morning glory, psilocybin, p-lsd, 25I-NBoMe |
|
Appearance |
White or off white powder, white or clear
crystals, capsules containing the drug, LSD – blotting paper squares, plant
seeds (morning glory and Hawaiian baby woodrose), dried leaves (chacruna) ,
magic mushrooms (psilocybin) |
|
Description: |
Substances which primarily alter cognition and/or
perception but do not have such a marked stimulant activity (like MDMA). Many
of the drugs of interest here are acting as agonists at serotonin receptors,
mimicking the effects of the naturally occurring brain chemical serotonin.
Some drugs such as ketamine are powerfully hallucinogenic, but have a very
different mechanism of action and are considered in a different category in
this briefing. |
|
Route: |
Varies with drug; swallowed or mucous membranes,
some are swallowed, DMT is smoked. |
|
Effects:
|
Will vary massively with drug, dose, setting and
user. Could include significant hallucinatory activity, feelings of profound
enlightenment or conversely intense paranoia. May enhance senses of sight,
sound and touch. Some can cause feelings of sexual arousal and increased
sensuality |
|
Risks:
|
Short term risk of significant panic, anxiety and
disorientation. Risk of accidents while intoxicated. Longer terms risks of
triggering or exacerbating mental health problems. |
|
Harm
reduction: |
Undertake research before using any such drugs to
establish risks, effects and dose ranges. Use only if in good physical and
mental health. Have a non-using friend on hand to help guide and manage
experiences. |
|
Dissociatives |
|
|
aka
dissociative anaesthetics |
|
|
Examples: |
Ketamine, PCP, methoxetamine, methoxphenidine, ether,
nitrous oxide, ether, salvia divinorum, tiletamine |
|
Appearance |
Ketamine, PCP and Methoxetamine take the form of
white, crystalline powders. Ether is a volatile liquid. Nitrous oxide comes
as a gas under pressure in small canisters or cylinders or as a propellant in
some foods (e.g. whipped cream). Salvia divinorum comes as dried leaves, or
powdered plant extracts. |
|
Description: |
Dissociatives fit in to the wider family of
hallucinogenic or psychedelics. They have distinctive characteristics partly
related to how they work, and how they are experienced. Unlike other
hallucinogens they are not working primarily on the serotonin system like
tryptamines. Instead they are believed to work in some cases by blocking NMDA
receptors in the brain or by acting as agonists at the k-opioid receptor. |
|
Route: |
White powder drugs like ketamine are snorted,
swallowed or less commonly injected. Volatile compounds such as ether or
Nitrous oxide are inhaled. Salvia is smoked, typically through bongs. |
|
Effects:
|
Reduced muscular control, paralysis, euphoria,
profoundly altered state, reduced sensitivity to pain, hallucinations,
hilarity, confusion and disorientation. |
|
Risks:
|
Risk of falls and accidents when intoxicated;
nausea and vomiting |
|
Harm
reduction: |
Use in safe environment with sitter; |
|
Deliriants |
|
|
aka
Tropane Alkaloids, Antihistamines |
|
|
Examples: |
Diphenhydramine, muscarine, atropine, scopolamine,
hyoscamine |
|
Appearance |
Plants such as Deadly Nightshade, Jimson Weed,
Datura, Thornapple |
|
Description: |
Deliriants are the most unpopular end of the
hallucinogen spectrum. They are unpredictable, can cause a lot of nausea and
are not especially pleasant. |
|
Route: |
Plant based products usually swallowed or taken
rectally. The powder based compounds such as benadryl can be swallowed or
snorted. |
|
Effects:
|
Significant hallucinations, confusion,
disorientation, drowsiness |
|
Risks:
|
Headaches, convulsions, shakes, tremors, breathing
problems, heart failure |
|
Harm
reduction: |
Don’t use any of the plant-based tropane alkaloids
– the level of risk is very high. |
|
Depressants (GABA-nergic) |
|
|
aka
benzos, Z-drugs, GHB, Barbiturates, downers, sleepers |
|
|
Examples: |
Benzodiazepines:
diazepam, temazepam, etizolam, phenazepam, flubromazepam, Nifoxipam,
deschloroetizolam |
|
Appearance |
GHB: liquid or white powder |
|
Description: |
These drugs act on GABA-receptors to reduce
electrical stimulation of the brain. Different substances have different
mechanisms of action. |
|
Route: |
Mostly used orally. Some benzos are soluble and
can be snorted. Some are prepared for injection. |
|
Effects:
|
Highly dependent on strength, dose and tolerance.
Low doses produce euphoria and relaxation, reduced motor control and decrease
in anxiety. Higher doses see further relaxation, possible amnesia, sleep and
possibly unconsciousness. |
|
Risks:
|
Combinations of these drugs, especially alcohol
with one of the others here, is a significant cause of fatal overdose. |
|
Harm
reduction: |
Don’t use for sustained periods of time; don’t mix
drugs within this family or with opiates. Seek medical help in withdrawal. Be
cautious of benzos or other net-sourced drugs. |
|
Depressants (Opioids and Opiates) |
|
|
Examples: |
Heroin, opium, codeine, morphine, dihydrocodeine,
buprenorphine |
|
Appearance |
White or brown powder (heroin) |
|
Description: |
Either drugs derived from the opium poppy
(opiates) or synthetic chemicals based on the same structure (opioids). |
|
Route: |
Depending on the user and the drug includes oral
administration, sublingual, smoked, snorted, injected and rectal. |
|
Effects:
|
Reduction in pain, sense of euphoria, calm and
well being |
|
Risks:
|
Addiction, overdose through respiratory
suppression, injecting complications, death |
|
Harm
reduction: |
Avoid use in combination with other sedating
drugs; use infrequently if not dependent; preferably use another route other
than injecting and if injecting practice safer injecting techniques. |
OTHER INFORMATION:
The
KFx website
Lots of resources here including screening and assessment tools. All are free to
download and can be reproduced for in-house use.
Psychoactive Substances Act Briefing
Synthetic Cannabinoid Briefing
Synthetic Cannabinoid Use Screening Tool
NPS Screening and Assessment Tool
Mephedrone Fact Cards
SCRA Fact Cards
More
sites:
The mainstream drugs education channels are way
behind the curve when it comes to novel compounds. So anyone seeking to educate
themselves about newer drugs will need to undertake a level of research
themselves. However, many of the sources of information are very biased:
anti-drugs, pro-drugs, run by manufacturers and so on.
Many sites will simply cut and paste information from
the same sources so it is important to try and gain information from a variety
of sites and critically assess it to gauge its validity.
The following sites have been useful in the
preparation of this and other resources:
|
Resource |
Description |
|
Drugs Forum |
Premier drugs discussion forum. High standards of
moderation and ratings for user comments ensure that poor quality information
and attempts to promote products are rapidly dealt with. If a drug isn’t
being discussed here it is probably not really available. |
|
Bluelight |
Very active drugs discussion forum. Hampered by
poor moderation and over-long threads which become unwieldy |
|
Erowid |
Long established drugs awareness website. Lots of
information about newer compounds but a little slow to update. |
|
Drugwatch |
Collective group of drugs agencies and workers who
produce briefings and collate information about new compounds. Website should
be forthcoming. |
|
DrugWise http://www.drugwise.org.uk/ |
Successor to Drugscope website |
|
Drugswheel |
Tool for understanding drug families and
up-to-date lists of legal status of newer compounds |
|
Crew2000 www.crew2000.org.uk/ |
Edinburgh-based drugs service with a great track
record of club and festival outreach. Lots of information and downloads on
newer compounds |
|
Neptune: |
Output from the CNWL
NPS project including this guide on clinical management of NPS. The guidance
doc is a 355 page tome! Essential reading – but very academic and a hard
read. |
|
Partyvibe http://www.partyvibe.com/ |
Forum which grew out of dance and club scene. Has
a lively drugs discussion section. Some very good contributions but lack of
moderation means it’s a bit of a field day for people promoting their wares. Plus,
now takes some dodgy adverts. |
|
PsychonautWiki |
Styled after Wikipedia
but focussed on NPS. Some good content but not clear how much scrutiny there
is of content. |
|
Snopes www.snopes.com/ |
Not a drugs website, debunks urban myths. When
drug myths (e.g. strawberry meth) do the rounds, a good place to check. |
|
WEDINOS: www.wedinos.org |
Welsh
emergent drugs testing service |
|
Wikipedia http://en.wikipedia.org/
|
On-line, user written encyclopaedia |
|
Why
Not Find Out |
Wesbite set up by the Angelus Foundation and Amy
Winehouse Foundation. Primarily interested in new compounds. |
|
What Martha Did Next |
Blog and campaign site set up up by Anne-Marie
Cockburn after her daughter Martha died following taking MDMA. Not much drugs
info but lobbies for harm-reduction and drugs education. |
|
Talk To Frank |
Government-funded website. Had improved its NPC
content lately but is not very detailed at this stage. Limited information
about a large number of drugs is now included. |
|
Journal of the DEA in the US. Highly detailed and
technical articles including chemistry of new and emergent compounds. |
|
|
EMCDDA |
The EMCDDA exists to provide the EU and its Member
States with a factual overview of European drug problems and a solid evidence
base to support the drugs debate. Produces regular reports about NPCs across the EU |
|
RedNet |
The Recreational Drugs European Network (ReDNet)
project is a multi-site research study with the aim of improving the level of
information available to young people (16-24) and professionals on the
effects of these new recreational drugs and the potential health risks
associated with their use. |
|
Psychonaut Project
http://www.psychonautproject.eu/ |
The Psychonaut Web Mapping Project was a 2-year
European Union funded project (January 2008 - December 2009) with the aim of
developing a web scanning system to identify and categorise novel
recreational drugs/psychoactive compounds, and new trends in drug use based
on information available on the Internet. |
Drug Facts:
@nticopyright KFx: redistribution on a not-for-profit basis: credit and link back to KFx site required