Social Media: 

 Website
Colour:
Website
Colour:
 -
-  -
-
Fact Sheet (PDF) | Facts Card: Image or PDF | Harm-reduction information: Image or PDF
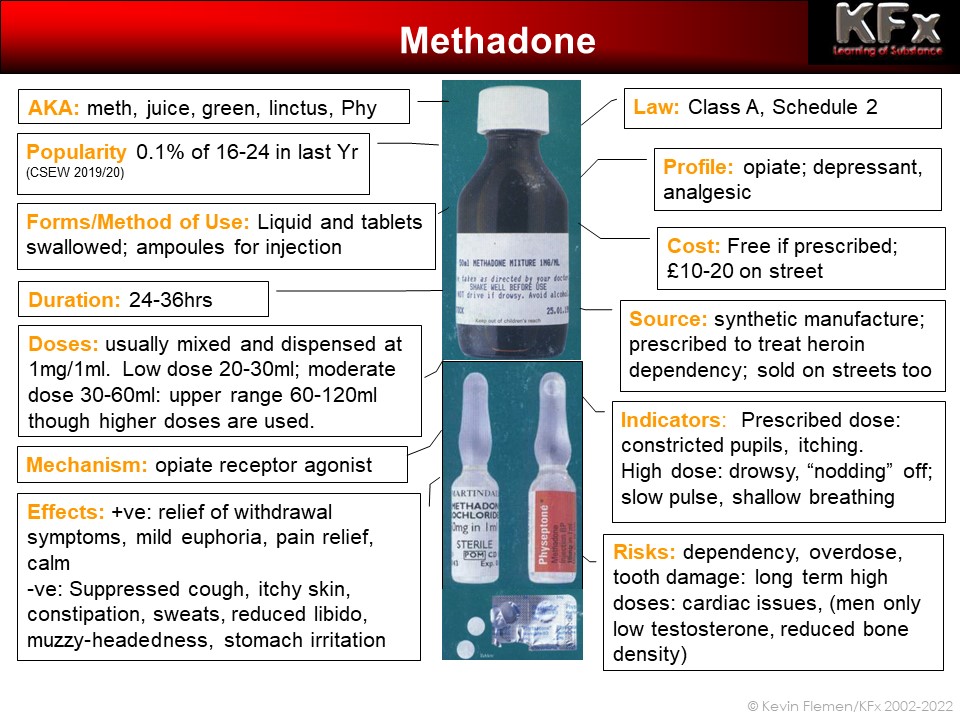
AKA: Methadone Hydrochloride, Physeptone, meth, Linctus, juice, amps
SOURCE: Prescribed drug, also sold illicitly
APPEARANCE: Liquid mixture, most frequently green, but also blue, orange, yellow or clear; Tablets; Ampoules for injection.
COSTS: When sold on the streets, ampoules typically sell for £20 or more, and are not relatively scarce as a street drug; tablets are increasingly scarce and could cost a few pounds each. Methadone Mixture is hugely variable in price at a street level - from £10 for a small volume up to £30 or £40 for a larger dose.
QUALITY: The issue of "quality" and "purity" is something of a vexed question when it comes to methadone.
Dispensed methadone will have a number of additives in it, potentially including dilutents, sweeteners, preservatives and colourants. Critics argue that some of these may be harmful - for example that sweeteners contribute to tooth damage,
Methadone comes in a variety of strengths. Methadone Mixture is most frequently mixed at 1mg/ml (i.e. 1mg methadone hydrochloride in 1ml of liquid).
Tablets: range of strengths, commonly 5mg or 10mg tablets.
Ampoules: Ampoules are usually mixed at strength of 10mg/ml. They come in a range of sizes and concentrations; some of the sizes are:
1ml (10mg),
2ml (20mg), 3.5ml (35mg) 5ml (50 mg)
Also available are concentrated ampoules, containing 50mg/ml.
Other strengths and formulations are available.
The active drug - methadone hydrochloride - is available in racemic form (where both the active levo-methadone molecules and the less active (or inactive) dextro-methadone molecules are also present.
In a small number of countries (e.g. Germany) levo-methadone has been prescribed, where the inactive d-methadone has been removed, leaving only the active l-methadone isomer.
Some commentators have argued that some people have difficulty metabolising out the d-methadone, and this causes some unpleasant side-effects in users. They argue therefore that the more-expensive l-methadone should be made more widely available.
However, a small number of trials have suggested that people transferred to and between different forms of methadone do not experience different withdrawal symptoms, once the relative strengths of the different compounds have been taken in to consideration.
METHODS OF USE: Methadone Mixture is designed to be taken orally; it contains additives which cause irritation and discomfort when injected. This irritation combined with the large volumes and associated vein damage make methadone an unpopular choice for injectors.
Tablets are also designed to be taken orally. However some users grind up tablets and inject them.
Injectable ampoules are intended for IM use; concentrated 50mg/ml were not originally intended for intravenous use, and can cause irritation and significant vein damage when injected in to a vein. Some users will dilute the ampoules to reduce the discomfort of injecting this highly acidic compound.
A single dose of oral methadone will start to work within around 30-60 minutes of consumption and reach peak levels after approximately three hours. Effects of a single dose typically last for around 24 hours, though, with regular dosing, the drug builds up in fatty tissue in the body and withdrawal effects may not start for around 36 hours after the drug has been taken.
EFFECTS: Methadone is a slightly less powerful painkiller than heroin, though it offers a similar, though less intense, absence of pain combined with moderately euphoric qualities. The combined effects are a sense of well being, feeling warm, and content, drowsy and untroubled. At higher doses, the user may become heavily sedated, be sleepy, unable to talk, and appear to fall asleep for a few minutes at a time.
Users often experience nausea or vomiting on the first occasions that they use methadone, or when returning to use after a period of abstinence. Side effects include suppression of the cough reflex, more shallow breathing and a slowing of the pulse rate. Some users experience intense, allergy-like itchiness. Other unwanted effects can include flushing of the skin, profuse sweating, reduction in libido, constipation, and confused thinking.
HEALTH IMPLICATIONS: Methadone is physically addictive. After a period of regular use, there is an unpleasant period of withdrawal (often called "cold turkey,") as the drug is cleared from the body and the body adjusts to functioning without the presence of methadone.
While unpleasant, sometimes lasting for two or three weeks, it is not a life-threatening process. Far more difficult is to resist the psychological temptation to use during this period, in the knowledge that it would instantly alleviate the symptoms of withdrawal.
Methadone remains in the body for longer than heroin, and many users assert that it is harder to withdraw from methadone than heroin. Regular use of methadone leads to an increase of tolerance to the drug. Initially, this means that one needs to take increasingly large amounts to achieve the same sense of euphoria and well being. Subsequently, it means that users find they need to use increasingly large quantities to prevent going into withdrawal, or just to feel "normal." Tolerance takes longer to develop than with heroin.
The flip-side of this is that, when methadone use is reduced (as with a reduction programme) or discontinued (for example after a spell in prison), tolerance drops. A user whose tolerance has dropped, who attempts to use the amount they were using when their tolerance was higher, stands a good chance of overdosing.
Overdoses where methadone is involved are not uncommon. Sometimes this involves methadone alone, but more often than not, it involves methadone in conjunction with other opiates (especially heroin) or methadone in conjunction with other depressant drugs such as alcohol or benzodiazepines.
When used as prescribed, methadone presents a low risk of overdose. However, when used by an opiate naïve individual, as little as 30-40ml could be fatal. Additional risks come where people use multiple doses of methadone at once, or use heroin on top of their prescribed methadone.
Methadone, like heroin, does cause severe constipation amongst regular users. In addition, it acts to suppress the cough-reflex, leaving users at risk of chest and bronchial problems.
Methadone can cause tooth damage, weight gain, perspiration and reduced libido, making it unpopular with many users.
Further health problems relating to methadone use stem from injecting. The injection of undiluted concentrated methadone ampoules has been linked to vein damage, tissue damage, ulceration and other problems.
PRESCRIBING MODALITIES: Guidance on methadone prescribing is provided by the Department of Health in the "Drug Misuse and Dependence - Guidelines on Clinical Management," the revised edition of which came out in 2007.
However, there is wide range of prescribing and dispensing practice in the UK.
Titration: Patients are typically started on a low dose which is then slowly raised until the person is 'correctly' prescribed - i.e. that they no longer experience withdrawal symptoms, but are not sedated. This process may take a long time, leaving patients in discomfort until their dose is increased, or increases the risk of dropping out of treatment.
Some regions have formal or informal upper-limits on dose ranges which means that some patients may be under-prescribed, experiencing withdrawal until their tolerance has dropped.
Supervision: In order to minimise leakage of methadone and to increase compliance with prescribing, patients are subject to various levels of supervision when prescribed methadone. This often includes daily supervised consumption - consuming methadone in the presence of the dispenser or daily pick-up - collecting daily but not supervised. Most people will need to pick up two day's worth at weekends.
In addition to supervision, many clinics will have some sort of testing regime in place to check for use of other drugs on top of methadone.
Maintenance or reduction: Many patients will be prescribed methadone with a view to becoming abstinent. To achieve this, patients are initially stabilised at a therapeutic dose then this is gradually reduced by small amounts over a period of time. By doing the reduction gradually, the worst of the withdrawal symptoms are meant to be avoided, and so the person eventually is "weaned off" methadone. If the process is done too rapidly, it is likely to be unpleasant.
Some people find that they lose their stability when they start to reduce, and so may be prescribed methadone on a maintenance basis - where the aim is not to achieve abstinence but to maintain stability. This open ended prescribing could take place over many years.
There is concern that some patients who could and want to be drug free are "parked" on methadone maintenance, whilst others, who are not ready to become drug free are reduced too rapidly.
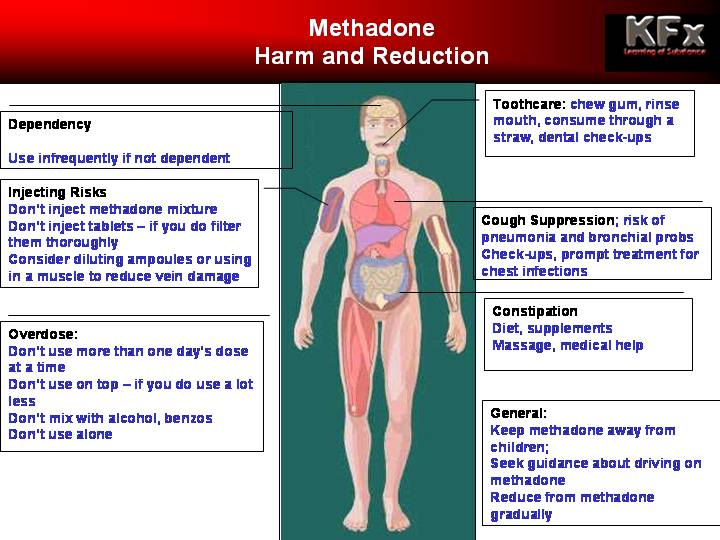
HARM REDUCTION: Mixing: Use of methadone with heroin or other opiates increases the risk of overdose. Patients receiving methadone should be advised of this risk and discouraged from using other opiates alongside methadone.
Where patients do use heroin or other opiates on top, it should be stressed that the person would need to use a lot less heroin than normal - or would be risking a fatal overdose.
Patients should also be advised that mixing other depressant drugs - especially alcohol or benzos - increases risk of overdose.
Dental care: Patients worried about dental health while using methadone could look at using a straw to take their methadone, chewing gum afterwards and rinsing mouth with milk or water. Discourage tooth brushing straight after use as the acid may have softened dental enamel. Consider use of sugar-free preparations. See a dentist regularly.
General health: maintain healthy diet and exercise to reduce weight gain exacerbated by methadone, and to improve bowel health and movement; increase fluid intake if experiencing substantial perspiration.
Children: don't allow children to get access to methadone; store it safely out of reach.
LEGAL STATUS: Methadone is a Class A, Schedule 2 drug. It can be legally produced, supplied and possessed under Home Office licence, but otherwise this constitutes an offence under the Misuse of Drugs Act.
OTHER INFORMATION: Methadone is predominantly prescribed as a substitute for Heroin, for those dependent on Heroin.
The advantages are that it is a pharmacological substance whose strength is known, and which can be delivered in precise doses. When prescribed as Methadone Mixture, it offers an oral route of administration, rather than by injection. When prescribed, it also offers an escape from the Heroin lifestyle by removing the need to fund a large heroin habit. Once receiving prescribed methadone, the user is also hopefully drawn into other services such as support, counselling and primary healthcare services.
The use of illicitly purchased Methadone negates many of the advantages of methadone use under a therapeutic regime. Problems of injecting, of the financial burden, an unwillingness to use agencies such as primary health-care, and increased risks of overdosing are all prevalent amongst those who use and become dependent on this pharmaceutical overspill.
Methadone is, in itself, an addictive substance and users can end up exchanging dependency on Heroin for dependency on Methadone.
Drug Facts:
@nticopyright KFx: redistribution on a not-for-profit basis: credit and link back to KFx site required
{kind=link}
{kind=link}