Social Media: 

 Website
Colour:
Website
Colour:
 -
-  -
-
Fact Sheet (PDF) | Facts Card: Image or PDF | Harm-reduction information: Image or PDF | Links | Resources
AKA: Amphetamine Sulphate: speed, whizz, sulph, billy,
phet, pink champagne,
Base Amphetamine: base, base speed, paste
Dexamphetamine Sulphate: Dexedrine, dexies, dex, Adderall
Methamphetamine Sulphate: Methedrine, Crystal Meth, meth, ice, shard,
glass, Tina, Shabu, Yabba, crank, Pervitin, Sisa
Benzphetamine: Didrex
The amphetamine "family" contains a number of prescribed and non-prescribed
stimulant compounds. Methylphenidate is related to amphetamines (though
not strictly an amphetamine.
PROFILE and RELATIVES: Amphetamines are a family of drugs, part
of the larger Phenethylamine group. The amphetamines are stimulant drugs.
Other relatives in the family include MDMA (Ecstasy) and the cathinones
(e.g. mephedrone).
There are a number of molecular variants of amphetamine, such as 4-fluoro-amphetamine.
Although not actually amphetamines, the drug Methylphenidate (Ritalin) has
very similar effects to the amphetamines and risks are similar. Analogues
of methylphenidate were briefly available on the UK market as they weren't
regulated but, in early 2015, they were brought under the Misuse of Drugs
Act.
ORIGINS: First synthesised in 1887, amphetamine only started to
get prescribed and used from 1934 onwards. It has been used in a variety
of settings including:
·Decongestant
·Weight loss
·Depression
·Military settings
SOURCE: Amphetamines are synthetic chemicals. There
are a number of production routes. Some amphetamines are synthesised in
clandestine labs in the UK, while the bulk of the rest is imported from
mainland Europe.
Ritalin is prescribed in the UK for the treatment of ADHD and some diversion does occur.
There is a limited amount of Dexamphetamine prescribing, including to people with history of amphetamine dependency. However, there is minimal leakage from such prescribing to the street.
Historically, in the UK in the 50s, 60s and early 70s, medical diversion of amphetamines was much more widespread. Benzedrine inhalers were broken open and the drug extracted. Dexamphetamine was widely over-prescribed for weight loss and diverted to the streets. Stimulants were also a target for pharmacy thefts. The now-notorious drug methamphetamine was originally a branded pharmaceutical product and was marketed in the UK as "Methedrine." It was briefly and unsuccessfully used in London as a treatment for cocaine dependency.
In Eastern Europe, when the Warsaw Pact was still in place, a brand of
methamphetamine called Pervitin was widely sold. As a term, Pervitin is
still used in a number of countries including the Czech Republic. A cheap,
crude form of methamphetamine, synthesised from ephedrine, has been reported
in the media as a cheap street drug in Greece, sold as Sisa.
APPEARANCE: The mainstay of the UK amphetamine market, amphetamine sulphate, is usually sold as a powder. Colour ranges from white, off-white, grey, yellow, and pink. It is usually sold by weight. This was typically in small rectangular wraps of paper, but increasingly now it is sold in self-seal bags. It is a sour-tasting, water soluble salt powder.
Increasingly commonly available is base-speed, a grey paste similar in consistency to putty or marzipan. It is a non-soluble base drug often smelling strongly of ammonia.
Dexedrine tablets are usually circular and are white or yellow. It is also
sometimes prescribed as a linctus.
Ritalin in tablet form is prescribed to children with ADHD and some of this
is diverted to illicit use.
Methamphetamine comes in the form of white powder or clear crystals, but
is also sold in tablet form, though tablets are less common in the UK.
QUALITY AND PURITY: Non-pharmaceutical products are highly variable in quality. Amphetamine sulphate powder in the UK is notorious for its low purity, typically between 5% and 10% pure.
Base speed, which was taken out of production earlier, tended to be higher purity, often around 40%. However, some suppliers made "fake base" by adding oil and ammonia to low quality speed powder to give it the look and smell of base speed.
Crystal meth, made in small batches and sold in crystalline form, is harder
to adulterate and tends to be higher quality.
COSTS: Speed is usually sold by weight, at a cost of around
£5 per gram. Base is more expensive, typically £20-40 a gram.
Methamphetamine: wide range of cited prices, from £50-200/g
DOSE RANGE: Hugely variable, partly influenced by drug of choice, purity, route, tolerance and experience. For amphetamine sulphate, doses of 100-200mg would be typical, but some will use way in excess of this.
ROUTES OF ADMINISTRATION:
Amphetamine sulphate: as a water-soluble drug, it can be readily snorted
or rubbed on gums. However, it has a very unpleasant taste and is painful
to snort so it is often wrapped in a cigarette paper and swallowed (bombed)
to get it in with as little taste as possible. Speed powder is also injected.
It requires no heating or acid but should be filtered (though rarely is).
Base speed: insoluble in water, though will melt in hot water. Injectors
have caused significant complications by heating base speed in water and
injecting it, where it tends to congeal on cooling. It is safer to dissolve
base speed in hot water and drink it. But if it is to be injected, it needs
to have an acid added to make a solution. It can be smoked.
Methamphetamine: a salt drug, which dissolves readily. It can be snorted,
rubbed on gums or injected without heating or addition of acid. Unusually,
although a salt, it can also be smoked.
Tablets: should be swallowed; if crushed for injecting should be filtered
thoroughly.
ONSET AND DURATION: Different members of the amphetamine family have different profiles in terms of duration of effect, and this will also change according to route.
Amphetamine Sulphate typically has a 2-4 hour duration of effect. Redosing
is common, with people dabbing top-ups in the course of the night to prolong
effects. Methamphetamine is longer acting.
Smoked and injected drugs will have a faster onset and shorter duration
of effects; swallowed drugs will come on more slowly and last longer.
MECHANISM of ACTION: Amphetamines have a number of mechanisms of
action. The key effect is to elevate levels of the brain chemicals dopamine,
nor-adrenalin (nor-epinephrine) and to a lesser extent serotonin. They do
this by:
Key physical effects include: Reduced appetite, Clenching jaws, Grinding
teeth, Elevated heart rate and blood pressure, dilated pupils, Increased
perspiration, nsomnia, talkative, repetitive,Restlessness, pacing
Key psychological effects include:euphoria, intense pleasure, confidence,
assertiveness, irritability, aggression, anxiety, panic, repetitive behaviours,
increased libido (but possibly reduced erectile function), tactile hallucinations
("bugs under skin")
INDICATORS of USE: The physical effects above are key indicators
of amphetamine use, but could also be caused by other stimulants.
Heavy prolonged use can result in nasal or tooth damage (depending on route),
weight loss, insomnia and mental health problems.
RISKS: Amphetamines can cause significant short, medium term and long term problems.
OD/Death: amphetamines put a significant strain on the cardiovascular system and can cause death through heart failure. Amphetamine was a feature in 120 deaths in the UK in 2013. This is low compared to opiates but the rate has increased year on year since 2010.
Weight loss: heavy prolonged use of amphetamines can cause significant and dangerous weight loss. In turn this can lead to organ damage, and compromised immune system.
Nasal/tooth damage: highly acidic amphetamine erodes and weakens teeth and, when rubbed on gums can cause tooth loss. It also irritates and damages nasal tissue when snorted. Smoked methamphetamine causes significant tooth damage leading to a condition called "meth mouth."
Swallowing amphetamine: although safer than other routes, amphetamine can irritate and damage the stomach lining and may cause stomach damage.
Risk taking behaviour: amphetamines can cause over-confidence, irritability and possible aggression. It can contribute to increased violent episodes, especially in night-time economy settings. Amphetamines can also increase libido and the use of methamphetamine in the "chemsex" scene has caused increasing concern. Chemsex is a term used to refer to drug-related sex activity, especially amongst Gay men, and is associated with the use of methamphetamine, and increased incidence of high-risk sexual activity.
Mental wellbeing: amphetamine causes an unpleasant comedown. Low levels of dopamine post use can cause low mood, depression, craving and dysphoria. Comedown also tends to leave the person feeling tired, run down, irritable and anxious. Even single episodes of use can lead to an unpleasant comedown - amphetamine is generally a drug that leaves the user feeling pretty low the next day. Some people will use other drugs (cannabis, benzos, alcohol) to take the edge off a comedown. Others will use more speed, leading to multi-day speed binges. The crash off extended use is inevitably far worse.
Amphetamines can cause anxiety and paranoia. With extended use, the combination of amphetamine use and sleep deprivation can lead to serious symptoms - hallucinations, delusion, paranoia and panic. The condition, often referred to as "amphetamine psychosis" doesn't usually persist once use stops and the person starts to eat and sleep again. However, symptoms can last for a number of days and possibly weeks, and may require inpatient treatment
DEPENDENCY: Amphetamines can and do lead to dependency. Patterns
of dependency in the UK are significantly different to other countries where
methamphetamine dependency is a more significant issue. Many drug projects,
especially in regions where there is entrenched amphetamine use, will have
a small cohort of speed-dependent clients.
Early speed use is euphoric, rewarding and typified by binges. Most people
learn to take long breaks from speed use and the unpleasant come-down is
a big deterrent.
After sustained, use, the person is liable to be significantly dopamine
depleted and feel very tired. At this point speed use is less about reward
and more about just being able to function. Speed becomes a tool to help
the person get up and do things.
A fair proportion of the dependent speed users attending drug projects are
older men, in poor physical health, who have been using for a number of
years. Some agencies also report seeing younger people who may have ADHD
who are self medicating with amphetamines some of whom have previously been
prescribed Ritalin.
Interventions don't usually require medical input, though some research
suggests use of anti-depressants to help reduce craving. The key interventions
centre on craving management, and interventions to address the low levels
of dopamine and the associated cravings.
Substitute prescribing isn't widespread in the UK but is still undertaken
on a limited basis.
MIXING: Amphetamine is used extensively alongside alcohol. The stimulant effects of amphetamine significantly reduce the sedating effects of alcohol, allowing for increased alcohol consumption. This increases the risk of alcohol related liver damage. Alcohol continues to disinhibit and the increased confidence and assertiveness of amphetamine with the disinhibition of alcohol makes for a volatile combination.
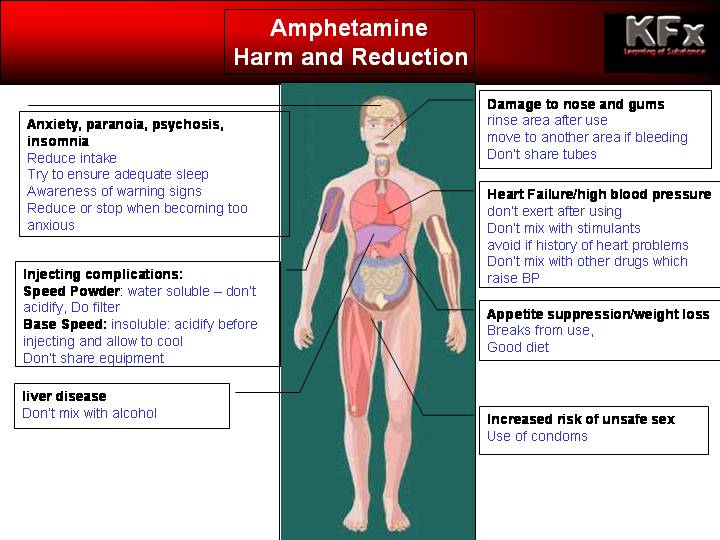
HARM REDUCTION:
Route specific harm reduction:
-don't share snorting or injecting equipment
-always practice safer injecting techniques
-discontinue application at site getting nose-bleeds or bleeding gums.
General health:
-don't use for extended periods of time - allow time to rest and recover
-don't use in combination with alcohol; if you do drink on speed moderate
alcohol intake and ensure adequate water consumption
-maintain diet or use liquid replacement meals
-consider use of vitamin D and calcium supplements
-avoid if you have high blood pressure or any family history of cardiac
problems
-be aware of indications of depression worsening mental health; discontinue
use and seek help.
TRENDS: According to the Crime Survey for England and Wales for
2014-15, only 1.3% of 16-24 year olds reported speed use in the last year.
This was marginally down on the previous year. Back in 1996 reported levels
were almost ten times higher, with 11.8% reporting use in the last year.
LAW: Amphetamines Sulphate is a Class B, Schedule 2 drugs. This
means that, unless produced, supplied or possessed under Home Office licence,
offences would be committed under the Misuse of Drugs Act 1971. Amphetamines,
like other class B drugs, are counted as Class A drugs when prepared for
injection.
Methamphetamine and other structurally modified Amphetamines (e.g. 4-Fluoroamphetamine)
are Class A drugs.
Pharmaceuticals such as Dexamphetamine Sulphate are legal if prescribed
and used by the person to whom they were prescribed. A small number of weaker
amphetamine-based compounds (e.g. Benzphetamine) are Class C drugs.
OTHER INFORMATION: Amphetamines were once one of the core drugs
on the UK drug scene. Recreationally they were popular in lots of music/club/youth
scenes and diverted amphetamines were popular with mods, rockers, Northern
Soul fans, and then a core feature in the punk scene and amongst some Goths.
Non-recreationally, amphetamines had long been a feature of the diet-pill
world. They were also used in a number of workplace settings, including
factory and warehouse work, fishing and driving settings, and amongst students
and night workers. Ian Fleming's James Bond uses Benzedrine on several occasions
in the course of work.
Speed has, in part been displaced by more popular, less harsh and more "glamorous"
competitors, most notably Ecstasy and cocaine. The advent of Ecstasy, with
a less edgy, more "loved-up" feel, made for a better clubbing
experience and contributed to a decline in speed's popularity. Where cocaine
was scarce and expensive, speed, although considered "poor man's coke"
was an acceptable alternative. As availability of cocaine increased and
price dropped, many people would choose to use cocaine over speed.
It had always been recognised that speed was a low purity drug at street
levels, and the advent of legal, pure alternatives like mephedrone and later
ethylphenidate contributed still further to a drop in speed's popularity.
Having said this, in large parts of the UK, speed remains the stimulant
of choice, especially where cocaine is hard to obtain. In an increasingly
contaminated "white powder" market, it's hard to know how many
of the street blends are, in part, amphetamine.
Drug Facts:
@nticopyright KFx: redistribution on a not-for-profit basis: credit and link back to KFx site required
{kind=link}
{kind=link}