Social Media: 

 Website
Colour:
Website
Colour:
 -
-  -
-
Fact Sheet (PDF) | Facts Card: Image or PDF | Harm-reduction information: Image or PDF |
| ABOUT THIS BRIEFING: This briefing provides an overview on Synthetic Cannabinoid Receptor Agonists It is not intended to provide detailed information on each compound or a list of all such compounds. The web version has no images in it; the downloadable PDF includes images,This version published8.1.19 to reflect legal changes, emerging SCRAs and evolving situation in the UK. |
This family of drugs work on cannabinoid receptors in the
brain and body, so are referred to as Synthetic Cannabinoid Receptor Agonists
(SCRAs). Although accurate, the term isn’t widely used outside of the
scientific community and so the term Synthetic Cannabinoids is often used as
it’s less of a mouthful.
When doing drug education, it is important to stress the
issues and risks with SCRAs are very different to plant-derived cannabis.
Participants should not get the impression that these products are just
synthetic versions of the chemicals in cannabis.
Drug Families include:
| “Classic Cannabinoids | HU-210 |
| Napthoylindoles: | JWH-004, JWH-018, AM2201 (etc.) |
| Naptheylmethylindoles | JWH-073, JWH-200 (etc.) |
| Naptheylpentylindoles | THJ-018, SDB-005, NM2-2201 |
| Napthoylpyrroles | JWH-398, AM-1221 |
| Napthylmethylindenes | AM-2201, AM-694, WIN-55,212-2 |
| Phenylacetylindoles | JWH-250, JWH-251, JWH-203, RCS-8 |
| Benzoylindoles: | AM-694, AM-1241, AM-2233, RCS-4 |
| Cyclohexylphenols: | CP-47,947 CP-55,940 |
| Cyclopropanoylindoles: | UR-144, 5F-UR-144, A-834,735, A-796,260 |
| Napthoylpyrroles: | JWH-307, JWH-147, JWH-030 |
| Adamantoylindoles | 5f-AKB-48, APICA, STS-135 |
| Indazole carboxamides | AB-PINACA, AB-FUBINACA |
| Quinolinyl esters | PB-22, 5F-PB-22 |
| [these lists are not comprehensive; there are hundreds of different SCs now on the market.] | |
For example compounds developed by John William Huffman in
America were given the initials
JWH, followed by a number (e.g. JWH-018.) HU-: Hebrew University
AM-: Alexandros Makriyannis
CP-: Carl Pfizer
Each compound has a long chemical name, possibly more than
one.
There is an “official” name based on an international naming
standard (IUPAC). But some drugs end up with unofficial names too, and
abbreviations derived from these unofficial names.
The names linked to the drug AKB-48 are a good example.
The ‘official’ name is:
1-pentyl-N-tricyclo[3.3.1.13,7]dec-1-yl-1H-indazole-3-carboxamide
but it is also known as
N-(1-adamantyl)-1-pentyl-1H-indazole-3-carboxamide.
This unofficial name led to an abbreviated name of APINACA
derived from its chemical name.
And why AKB-48 in the first instance? Possibly because it
was derived from an earlier compound called AB-001. AKB-48 was first reported
in Japan in 2012 and there’s a Japanese girl band called AKB-48 so maybe it was
named after them. Who knows?!
Overview – “potted” history: Synthetic cannabinoids have
been on the market since around 2007, but for a fair while their presence
wasn’t widely reported. “Herbal smoking mixtures” such as Spice or Aztec Gold
were offered by head-shops and on-line sellers as an alternative to cannabis.
This, in turn was nothing new. Head-shops had, for years
been selling “smoking mixtures,” usually a mixture of plant material with
loosely psychoactive properties. Such mixtures generally resulted in a
headache, sore throat and a house that smelt like an autumnal bonfire with
little if any psychoactive effects. The newer compounds like Spice were
different – they worked and so interest and use started to increase.
Analysis of samples of Spice revealed that, rather than
being a blend of herbal smoking mixtures, the products were inert plant
material, which had been sprayed with a synthetic cannabinoid (initially
JWH-018) – a chemical which mimicked the action of THC or CBD at cannabinoid
receptors in the brain.
These synthetic cannabinoids were originally being used in
research settings. They were synthesized by researchers in different settings –
such as compounds developed in the mid-eighties by John Huffman. It was a
couple of these, including JWH-018 which cropped up in the Spice and Aztec Gold
smoking mixtures.
This was made a Controlled Drug in 2009, but a new product
“Black Mamba” emerged, which contained AM-2201 which in turn was made a
Controlled Drug in 2013.
After this, and up to the Psychoactive Substances Act (2016)
the market expanded, more and more branded products appeared including
Pandora’s Box, Exodus Damnation, Cherry Bomb, Sensate, Vertex and many others.
These branded products included the next wave of SCRAs,
especially AKB-48, 5F-AKB-48 and PB-22. These, and other chemicals, were
designed specifically for the “legal highs” market rather than being repurposed
from research.
The Psychoactive Substances Act brought an end to these
branded products, as there were no longer legal avenues for sale such as
headshops.
Illegally imported and distributed synthetic cannabinoids
continues to enter the UK and is now generically referred to as “spice” or
“mamba,” a reference back to the earlier branded products but containing
different chemicals.
Time-line and Law: The range of synthetic cannabinoids on
sale in the UK has changed several times. In order to address each emergent
group of drugs, amendment were made to the Misuse of Drugs Act but, predictably
newer (and frequently more toxic) compounds emerged that were not covered,
requiring further legislative changes.
There have been three (or four) “generations” of
cannabinoids, and within each “generation” a range of different compounds have
been available.
The majority of SCRAs are covered by the Misuse of Drugs Act
by one of the 2009, 2013 or 2016 amendments. However, the legislation is now
complex and requires a good understanding of the molecular structure of newer synthetics
to be certain if they are covered by the amended legislation.
|
|
Date |
Key Compounds |
Products |
Legality |
|
1st Generation |
2007-2009 |
JWH-018 |
Spice Gold |
Class B CD December 2009 |
|
2nd Generation |
2010-2013 |
AM2201 |
Black Mamba |
Class B CD [HO Circular |
|
3rd Generation |
2013-2016 |
AKB-48, 5F-AKB48 |
Pandoras Box |
Class B |
|
4th Generation |
2016... |
5F-ADB (also known as 5F-ADB-PINACA) (and many others) |
“Spice” |
Some of the fourth generation SCRAs are not covered by the MoDA but will
fall under the PSA (2016). |
The Government had toyed with creating a novel definition to
address synthetic cannabinoids by creating legislation that reflected where the
drug worked rather than its chemical structure. The idea was that any drug that
acted as a CB1 receptor agonist would have been covered, but, for reasons
unknown, the Government appears to have abandoned this legislative route,
preferring to use the PSA instead.
Current Market [January 2019]:
Currently on sale on Dream Market | ||
| 4Cn-BINACA-ADB | 5F-MDMB-2201 | 4F-ADB |
| MAB-CHMINACA | 5C-AKB-48 | 5F-ADB (5F-MDMB-PINACA) |
| SGT-67 | SGT-78 | SGT-263 |
| AMB-CHIMANACA | THJ-2201 | M-PHP-2201 |
| FUZ-AMB | FUB-EMB | FUB-2201 |
| NM-2201 | JWH-X18 | 4-BB-22 |
| 5C-APB | PP-ADB | PY |
| SDB-001 | 5F-AXB | 5CL-ADB-A |
| ADB-FUBINACA | SGT-151 | |
| 5F-CUMYL PINACA | 5,3-AB-CHMFUPPYCA | |
| Notifications from EMCDDA | ||
| 5F-AKB-57 | Cumyl-CH-MeGaClone | 4F-MDMB-BINACA |
| 5F-AB-P7AICA | WIN-35428 | MPhP-2201 |
| AMB-4en-PICA | DMBA-CHIMANACA | MBA-CHIMANACA |
| MMB-FUB | MMB-022 | EG-018 |
| SGT-151 | 5F-SGT-151 | |
We have better monitoring now of hospital admissions and
deaths but it’s unclear if increases in figures are a result of more incidents
or better recording and monitoring of such incidents.
According to the CSEW around 1.2% of 16-24 year olds
reported use of NPS in 2017-18, unchanged from the year before. 33% of those
who had used and NPS said it was a “herbal smoking mixture.”
However, the CSEW is a poor tool for assessing SCRA use as
it excludes prisoners and homeless populations, the two key demographics where
use of SCRAs is widespread.
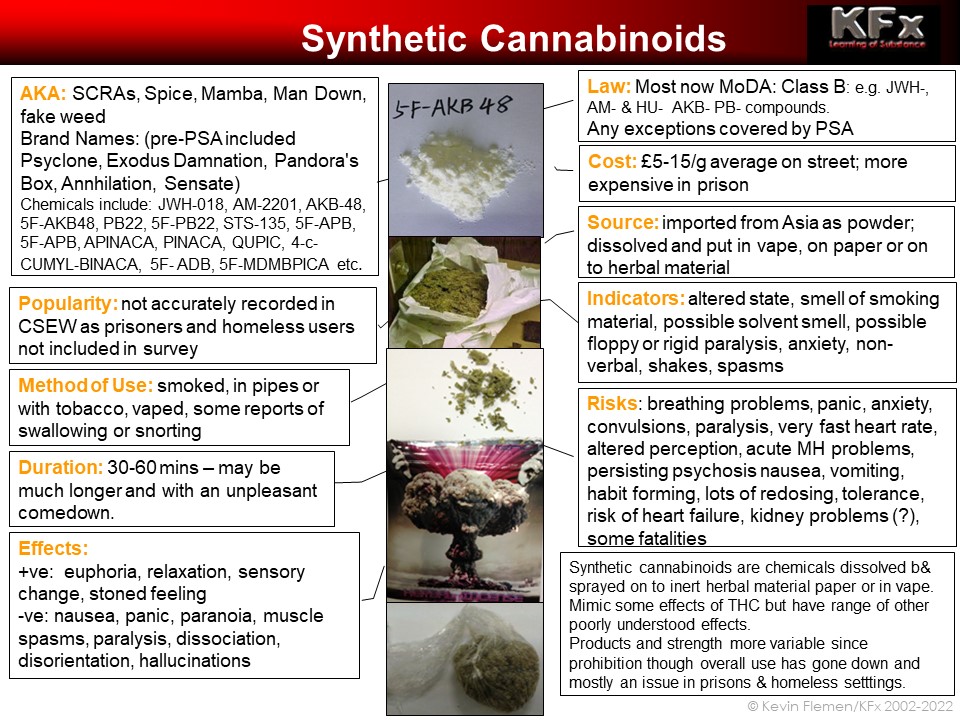
SOURCE: Raw “spice powder” is produced in overseas
laboratories for non-scientific use. Imported in to UK directly from
manufacturers or via Dark Web drug markets then prepared for street sale.
There have been claims, especially in custodial settings,
that home-made “spice” has been made in domestic setting in the UK out of
household products. These claims are highly dubious: while some of the earlier
SCRAs were relatively easy to make, the precursor chemicals are not household
products or readily available. Claims therefore that “spice” can be made in
Prison workshops are therefore not credible,
APPEARANCE: Synthetic cannabinoids are sometimes available
in street settings in a ‘raw state’ as crystalline white or brown powder though
this is not the most common form. This would be very potent and would in turn
be mixed with tobacco or another smoking mixture for consumption. Deaths
occurred in Manchester where raw SCRA was sold mistakenly for MDMA, and taken
in fatally large doses.
Raw spice powder: as sold on-line via Dark-web retailers.
Average potency of 1g herbal spice is 10mg 5F-ADB. So 1g
5F-ADB makes 100 average doses. Each 1g bag sells for £5-10.
Wholesale price: 1000g @ £2500. £2.50/g. Makes up 100,000
doses, around £500,000 worth of street drugs.
UK retailer. 50g @ £728/g £14.56/g. 5000 doses at £5/dose =
£25,000
The imported spice powder is dissolved in a solvent, usually
acetone and sprayed onto an organic herbal material for sale.
In liquid form it can also be used to impregnate paper for
sending in to prisons or sold in diluted liquid form for vaping.
COSTS: Street deals of herbal “spice” sell for £5-10/g. In
custodial settings prices can be much higher.
COMPOSITION, QUALITY, STRENGTH and DOSES:
As with all illicit compounds, the person using the
substance can never be certain what they are taking.
This is certainly the case with synthetic cannabinoids. The
active chemicals sold in the UK have changed several times and so users cannot
be certain:
• Which
chemical or chemicals are present on the product they have bought
• The
concentration/quantity of drug on the material.
One product containing AMB-FUBINACA contained 1.2% drug while
another sample contained 4.5%. This sort of variance, in the same City in the
same month, goes some way to explaining how easy it is for unwitting users to
take more of a drug than intended, or be given a substance that is unfamiliar
to them.
A year later, further research in Manchester showed that the
substances on sale in 2017 had largely vanished from the market. 24 of 26
samples instead contained the drug 5F-ADB. Again, doses varied massively:
0.19mg/g to 37.8mg/g with a median of around 10mg/g.
These results are location and time specific and no similar
research has been undertaken and made available in the UK so we do not know the
composition or potency of much of what is sold in the UK as Spice or Mamba.
Having said this, even if people knew which products they
were specifically were using, the lack of detailed information about
differences between specific products would mean that additional
substance-specific harm reduction information would be thin on the ground. We
can only talk in general terms about synthetic cannabinoids at this stage.
Synthetic cannabinoids are often much stronger than their
natural counterparts. Starting doses need to be much smaller. Different
synthetic cannabinoids vary dramatically in terms of potency. Different blends
of spice/mamba will vary in terms of the drugs that they contain and the amount
of drugs on the smoking material.
It is therefore essential to start with a very low tester
dose to assess strength of each batch. Increase doses very cautiously. The gap
between a tolerable dose and an overdose may be very narrow.
• Starter
doses to assay strength and for those unfamiliar with synthetics should be no
bigger than the head of a match. This should be mixed in with smoking material
but NOT herbal cannabis. If being smoked in a pipe or bong, even smaller
quantities may be indicated.
• Potency
may increase as people get to the bottom of the bag. If the psychoactive
material is not firmly bonded to the smoking mixture, it can lead to “bottom of
the bag” syndrome, where active ingredients can shake off and become
concentrated in the bottom of the bag and can be unexpectedly potent.
There have been warnings from Police, custodial settings and
drugs agencies suggesting that synthetic cannabinoids have been adulterated
with opiates and claims that fentanyl-family drugs have been added. These
suggestions have not been confirmed by toxicology reports and so suggestions of
“fentanyl in spice” should be treated with great caution and not recirculated
without confirmation. Critical incidents related to SCRAs are more likely to
stem from taking a large quantity of a potent SCRA or using a stronger product
than expected than from the addition of fentanyl.
METHODS OF USE: In community settings synthetic cannabinoids
are usually smoked as spliffs – mixed in with tobacco and smoked. As very small
quantities of synthetic material are required to achieve intoxication, smoking
“straight spliffs” of smoking mixture alone without tobacco is not recommended.
Synthetic cannabinoids and are also used in pipes and bongs.
Given their relative potency and the small quantities needed to achieve
intoxication, care is needed when using pipes or bongs to avoid unpleasant
overdose experiences.
With an increased availability of e-liquids some people will
vape rather than smoke their synthetic cannabinoids. This has also happened to
some people inadvertently. There have been some cases of people buying CBD
e-liquid (which would be legal and have little if any psychoactive effects) but
finding that the liquid contained Synthetic Cannabinoids (illegal and highly
psychoactive.)
As tobacco-free initiatives have been rolled out in Prisons,
prisoners have adopted new techniques. This has includes adding spice to dried
teabags (especially mint tea according to several sources) or “adapting” the
chamber of e-cigarettes to allow the use of spice in liquid forms.
Anecdotal reports of snorting and injecting raw Spice powder
have not been substantiated. Given the rapid, high levels of intoxication
achieved through smoking and the poor water solubility of most of the synthetic
cannabinoids currently on the market, it seems unlikely that snorting or
injecting would be very efficient.
There have also been a small number of reports of synthetic
cannabinoids being used orally but this does not seem to be commonplace.
MECHANISM OF ACTION: We do not fully understand how
synthetic cannabinoids work, or all their points of action.
THC is one of the naturally-occurring chemicals present in
herbal cannabis and cannabis resin. It is involved in the euphoria associated
with cannabis use but may also be involved in less pleasant effects such as
panic, paranoia and mental health problems. In ‘traditional’ strains of
cannabis, THC is joined by other compounds including CBD, which is believed to
play an important role in the anxiety-reducing, relaxing effects of cannabis.
THC and CBD bind to and activate cannabinoid receptors in
the brain – CB1 and CB2 receptors.
Early emergent chemicals, such as HU-210 were primarily
active at the CB1 cannabinoid receptor and demonstrated much higher levels of
affinity for these receptors than “natural” THC from cannabis plants. Some
synthetics are thought to be 100 x the
strength of THC. They may also have different affinities – binding more selectively
to receptors in one part of the brain or body rather than others.
Later generations of synthetic cannabinoids act at CB1
receptors but may also interact with other brain processes. This could include:
• Possible
impact of adamantine-related chemicals on dopamine levels
• Possible
blocking of glutamate receptors, leading to ketamine-like dissociation,
paralysis, and hallucinations
• Possible
interaction with serotonin receptors via indole-derived drugs.
We know little about how newer synthetic cannabinoids work.
We know still less how they work in combination, how they are metabolized, and
how these processes will be affected by the presence of other drugs.
EFFECTS: The strength and composition of street synthetic
cannabinoids varies significantly. It is not surprising therefore that the
users experience can also vary. The mental wellbeing of the user, other drugs
taken at the same time, the setting and other variable can also make for an
unpredictable experience.
The sought-after effect is a euphoric, stoned, detached
feeling. This could include altered perception, hilarity and a feeling of
relaxation and calm.
Many users report unpleasant symptoms instead including
anxiety, feelings of panic, disorientation and dysphoria – the opposite of
sought-after euphoric feelings.
Some of these effects are probably an individual reaction to
a specific drug or mix of drugs. For other people it is an ‘overdose,’ taking a
larger amount than the person can cope with safely or enjoyably.
Unpleasant effects/risks:
Reported key effects/side effects of current synthetic
cannabinoids include:
• very
severe panic,
• fear-generated
aggressive responses
• paralysis,
rigid limbs
• uncontrollable
limb movements
• convulsions
• inability
to communicate
• profound
hallucinations, including believed death experiences, detachment,
depersonalization, derealization
• highly
altered, delusional states (some of sufficient severity to warrant admission to
psychiatric wards as acute patients,
• very
fast heart rate, and conversely very low heart rate
• respiratory
distress following use including tightness of chest and tightening of the
airways,
• loss
of feeling and numbness in limbs,
• reduced
sensitivity to pain
• impulsive
behaviour
• loss
of consciousness
• amnesia
post incident
• elevated
body temperature
• nausea
• vomiting
• loss
of bodily functions
Reported in the past but not so many reports recently:
• kidney
problems (associated with some batches in New Zealand primarily)
• severe
coughing including coughing up blood (historic reports)
Associated with withdrawal:
• nausea
and vomiting
• stomach
and bowel pain
• shakes
and sweats
According to the ONS, Synthetic Cannabinoids were recorded
for 11 deaths up to and including 2015.
The total number for 2016 and 2017 was 51. This may be an
under-estimate as synthetic cannabinoids won’t show all show up on a routine
toxicology screen and additional, expensive analysis will only be requested
when there are grounds to do so.
The Prison Ombudsman notes 64 deaths in custody between 2013
and 2016 – a higher number than that recorded by the ONS. It notes 44 of these
were “self-inflicted” and includes self-harming when intoxicated or suicide.
Nine deaths were attributed to direct toxic effects (e.g.
heart failure, convulsions).
Dependency: Many
users, especially less constant users in prison find that they can move off
synthetic cannabinoids once their environment changes i.e. when removed from
ready access to spice in prison and the pressures to use in a custodial environment.
However, a smaller number of prisoners and homeless users
describe physical and psychological dependency.
With regular, frequent use tolerance can develop, leading to
escalating doses. With heavy use withdrawal symptoms have been reported including:
• intense
craving
• hot
and cold spells
• sweating
• stomach
cramps, bowel pain
• dry
heaving, nausea and vomiting
• irritability
• insomnia
• paranoia
and anxiety
• neuralgic
pain
• shakes
tremors
Treatment for dependency
There is no clear protocol for treating dependency on
synthetic cannabinoids, and the limited available literature stresses the
relevance of psychosocial interventions and holistic support as with other
patters of drug dependency.
The Project Neptune report on the Management of Synthetic
Cannabinoids says that symptomatic management of withdrawal symptoms may be
indicated.
Synthetic cannabinoid users, especially those who are street
homeless are likely to have multiple needs that will need to be addressed
alongside dependency. This could include:
• Homelessness,
• Poor
self-esteem and sense of self-worth: public and media perception of
“spice-zombies” is likely to reinforce feelings of low self-worth and lack of
capacity to change,
• Poor
mental health,
• Challenging
behaviour when intoxicated.
Joined-up interventions between outreach services, housing
providers, drugs and mental services will be essential to provide a safe,
therapeutic environment where dependent spice users can start to engage with
services.
The KFx website has two resources exploring treatment.
The Synthetic Cannabinoid Toolkit can be used over a series
of sessions to assess for dependency, develop motivation and plan change. It can be downloaded from here:
Where physical dependency may be a significant issue, the
Synthetic Cannabinoid Withdrawal Severity Index is intended to assess common
withdrawal symptoms and look at potential interventions including medical
management of symptoms. It can be downloaded here:
Long term risks:
As the latest synthetic cannabinoids have only been
available for a couple of years at most, we don’t know enough about long-term
risks and if these drugs will significantly increase risks of illness in the
future. We don’t know if the drugs will turn out to increase risk of cancers or
other organ damage. Although there is no research evidence either way, any
health risks are likely to increase with longer-term, heavier use so
common-sense advice would be to use at lowest dose for the shortest period of
time, and wherever possible reducing and stopping use.
We also don’t know the impact of SCRA use during pregnancy,
but again the best advice would be to avoid using during pregnancy and seek
help if abstaining from SCRA use during pregnancy is difficult or a detox is
required.
There is some evidence of long-term kidney damage linked to
SCRA use. It is unclear if this was a direct consequence of the drug or solvent
used in the preparation of the drug.
There have been reports of stroke-like symptoms after SCRA
overdoses, possibly linked to impeded blood-flow during seizures. There is no
published literature on this health issue.
Anecdotal evidence suggests that SCRA use is associated with
poor mental health outcomes. Many users experience acute psychotic episodes
during use, which usually resolve within 30-60 minutes but may persist for a
few hours and in exceptional cases symptoms may persist for 48 hours or so.
There have been reports of chronic mental illness after SCRA
use: this may have been over a sustained period of use but there have also been
non-corroborated accounts of people experiencing long term mental health
products after only brief experience of SCRA use.
It is not clear if these outcomes are caused by SCRA use
causing the development of a mental illness in novo or if the drug is
triggering or exacerbating an existing condition.
We do not yet know if use amongst young people will increase
the risk of psychotic-type illness, as heavy use of strong cannabis appears to.
However, it would not be unreasonable to assume such a correlation will be a
risk.
During acute episodes of spice intoxication, users can
experience very high levels of panic and distress and may have a partial memory
of the traumatic experience. However, as use is often associated with amnesia
any recollection is likely to be incomplete. Some SCRA users describe
flashbacks and moments of panic after using and it could be that these are akin
to PTSD. The term “chemical-induced PTSD” could describe the flashbacks caused
by delusional traumatic experiences caused by Spice, which the user can only
partially recall after the event.
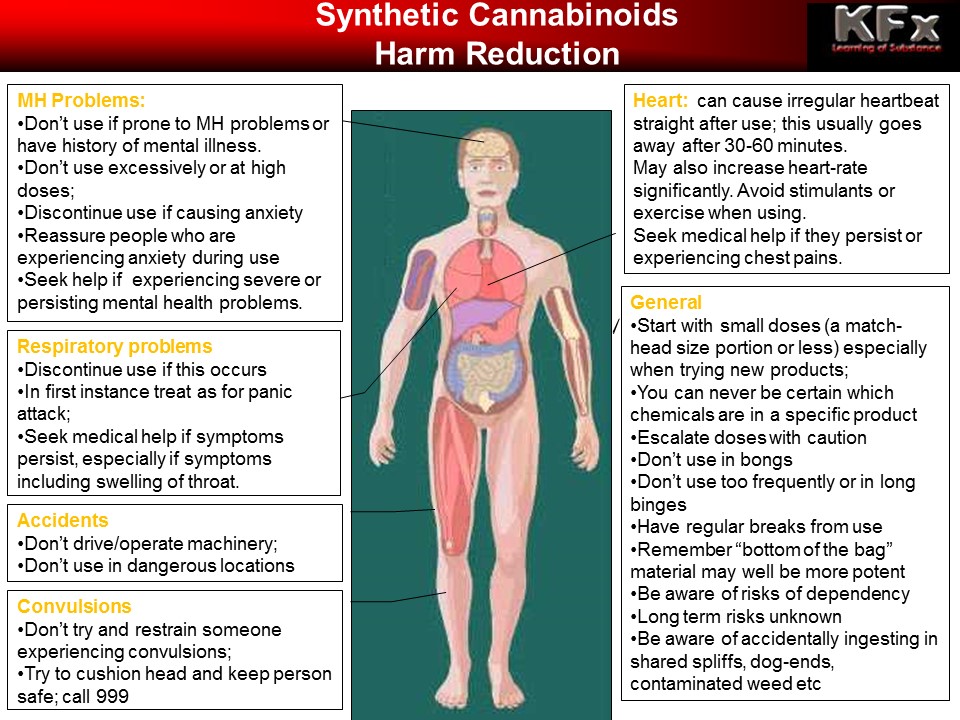
REDUCING HARM:
The scope for detailed harm reduction is hampered at present
by:
a) A lack of
information about which chemicals are present in any given batch of ‘spice’ on
the streets and
b) Even if
we did know which chemicals are present the lack of information about the short
and long-term risks of these chemicals, and how they may interact with other
substances.
It is not therefore possible to suggest if any of the
various substances on the market are more or less safe than others. Likewise,
we can’t speak with any certainty as to how safe or unsafe products may prove
to be in the medium to long term.
In lieu of more detailed information only the broadest of
harm reduction messages can be offered, including the following:
There have been numerous reports in custodial and street
settings of oranges, orange juice or sugar water being used to “treat” spice
episodes. An urban myth seems to have emerged that the vitamin C in orange
juice can help reduce the severity of episodes.
This may have been linked to the use of sugar solution in Dutch coffee
shops to treat cannabis ODs or the urban myth that Vit C shortens LSD bad
trips.
If someone is having a bad reaction to synthetic
cannabinoids but is still lucid, can communicate and sit up, then having a
sugary drink to sip may help. However, if the person is delusional, having
difficulty sitting up, and may be at risk of convulsions or is having seizures,
then nothing should be placed in the mouth and attempting to give fluids at
such times could result in choking or flooding the lungs. Do not attempt to
give juice or water to people experiencing such symptoms.
There have been anecdotal reports of naloxone being used
during SCRA-related episodes and reputedly ending the episode. This has variously
been attributed to potential action of SCRAs at opiate receptors, SCRAs cut
with opiates (for which there is no evidence), dual use of opiates and SCRAs
(where the naloxone is blocking the opiate action not the SCRA), or some other
mechanism yet unknown.
Where there is reasonable belief or grounds to think the
casualty is experiencing an opiate overdose then naloxone should be deployed if
available.
In other situations where there is a non-responsive casualty
with critically-reduced respiration, Emergency Services should of course be
called. First Aid interventions including rescue breaths and CPR may be
required, and advice from emergency call handlers can be sought, including
whether to deploy naloxone.
Testing/detection: Urine immune-assay tests were developed
for first generation SCRAs but became obsolete rapidly when the products on the
market changed. Testing companies were understandably hesitant about developing
tests for second generation compounds fearing that any such tests would also become
redundant.
Tests for third generation SCRAs are available and were able
to detect many of the SCRAs on the market around 2014-15. However they weren’t
able to detect all SCRAs. In one piece of research conducted in prisons, “dip
and read” tests of over 500 samples showed positive results 1.7% of the time.
The same samples subjects to LC/MS analysis in a laboratory revealed 20.2% of
samples were positive for SCRAs, highlighting the poor sensitivity of urine
testing.
As new compounds have emerged since this research, it is
likely that older tests will be still less accurate with emergent SCRAs.
Some prisons have been using ion-track machines to test
letters and swab prisoners. These can detect some older synthetic cannabinoids
but again may not be up-to-date with emergent compounds. Several prisons have
been perplexed at finding no drugs showing up on the ion-track but getting
positive results for acetone. This led to the erroneous belief that prisoners
were simply using acetone to “get high.”
It is more likely that the machines were able to detect and
match acetone to the database and showed positive results for this but couldn’t
do the same for the novel SCRAs presenting the false impression that there was
just acetone present.
Acetone is highly volatile, and so paper soaked in acetone
will dry out rapidly leaving only traces of acetone behind. There would be no
intoxicating effects of smoking paper with traces of acetone on it.
Folk Devils and Moral Panics: The Psychoactive Substance Act
removed legitimate synthetic cannabinoids from the Head Shop shelves, and in
doing so eradicated the labelled, regulated trade. This reduced access to young
people and recreational users. Overall the demand and use for synthetic
cannabinoids is very low. Of the 20,000 plus entries for cannabis products on
one Dark-Web drug market, less than 300 are for SCRAs. Given the choice most
people prefer traditional cannabis. Spice and Mamba have become the preserve,
almost exclusively or homeless and incarcerated users. For the suppliers there
is enough demand and profit in these small markets to warrant importing and
distributing the drug. For the users, the oblivion provided by SCRAs is worth
it, in lieu of other drugs, to escape the unpleasant environment of street
homelessness or prison.
The use of Spice in community settings is inextricably
linked to homelessness. There has been a well-documented correlation between
homelessness and drug use and as the former has increased in the UK over the
past few years, so too has the level of drug use amongst people in housing
need. And one of the affordable, available drugs in some areas remains Spice.
In previous generations this cohort would have been more likely to develop
opiate habits. In some cities this time, SCRAs have become the go-to drug
instead. It has the advantages of low cost, high availability and no need to
inject it. In some cities where spice is less available, workers and housing
providers have seen a reversion to heroin use amongst street homeless
populations.
The highly-visible phenomenon of people intoxicated with
SCRAs in public places has led to a massive level of pejorative media coverage.
References to “spice” as a “zombie drug” and pictures of people paralysed and
apparently insensible in the street have created a sense of a spice epidemic
out of control.
In turn this reporting has reinforced the sense that
synthetic cannabinoids are something that we don’t understand, can’t respond to
and can’t manage. In the same way that crack users in the early 90s were
demonised and excluded from housing and other services, so now spice users are
the new untouchables.
The lack of resources, combined with the social stigma
associated with spice use contribute in turn to poor self-esteem, lack of
self-worth and make engagement with services still more difficult.
Services are starting, slowly, to develop holistic responses
for people with multiple needs who use synthetic cannabinoids.
FURTHER INFORMATION:
Spice Boys: In 'Spice Boys', VICE reporter Ben Ferguson travels
to Manchester to meet some users who have become addicted to over-the-counter
substances. [made pre-PSA but highlights addictive nature of SCRAs]
Drugs Map of Britain: Wolverhampton: getting off Mamba
[2016]: In the first of our landmark new series looking at drug use across
Britain, we explore a legal high epidemic in Wolverhampton. Following
27-year-old Liam over three months in his battle to quit the synthetic
cannabinoid black mamba.
Spice: Synthetic Cannabinoids (SCRAs) [2017]: Linnell
Publications/Manchester City Council/NHS Manchester CCG
Harms of Synthetic Cannabinoid Receptor Agonists (SCRAs) and
Their Management: Neptune: 2016
“The main objectives of the study were to determine drug
misuse patterns for public health monitoring purposes and to inform healthcare
commissioning intentions. The study also
provided an opportunity to review the effectiveness of the ‘Spice’ point of
care immunoassay screening test that was at the time being widely used across
the prison estate to test for the use of synthetic cannabinoid receptor
agonists (SCRAs).”
Spice Users are Becoming a Cruel Online Joke: Vice (Max Daly) A growing
number of sites have become dedicated to posting 'funny' videos of the victims
of Britain's Spice epidemic.
Drug Facts:
@nticopyright KFx: redistribution on a not-for-profit basis: credit and link back to KFx site required
{kind=link}
{kind=link}